
Methylphenidate vs Ritalin: Key Differences, Clinical Uses, and Side Effects Explained
Abstract
Methylphenidate vs Ritalin: both medications are central nervous system stimulants used primarily to treat ADHD by increasing dopamine and norepinephrine levels in the brain. While they share similar therapeutic effects and side effect profiles, differences in formulation and onset of action can influence their efficacy and tolerability. Knowledge these distinctions is crucial for optimizing treatment outcomes and managing potential adverse effects.

Methylphenidate in 3 Minutes. Methylphenidate vs Ritalin
Methylphenidate vs Ritalin: Understanding the Drug and Its Uses [1]
Methylphenidate is a synthetic compound that belongs to the classes of substituted phenethylamines and phenidates. Chemically, it is built on a phenethylamine backbone, which includes a phenyl ring linked to an amino group (-NH₂) through a two-carbon ethyl chain. It shares structural similarities with amphetamine, especially due to a substitution at the Rα position that is integrated into a piperidine ring ending at the terminal amine of the phenethylamine structure. Moreover, a methyl ester group is attached at the Rβ position, contributing to its pharmacological activity.
This compound is a central nervous system stimulant that works by increasing the levels of dopamine and norepinephrine in the brain. By enhancing these neurotransmitters, methylphenidate improves attention, impulse control, and overall cognitive processing—effects that make it particularly effective in treating Attention Deficit Hyperactivity Disorder (ADHD).
Ritalin is a brand-name medication whose active ingredient is methylphenidate. In other words, Ritalin is a specific pharmaceutical formulation of methylphenidate. It is one of the most well-known and commonly prescribed drugs for ADHD. Ritalin helps manage symptoms such as inattention, hyperactivity, and impulsivity by boosting activity in parts of the brain that control attention and behavior.
In addition to its approved medical uses, Ritalin has been used off-label by individuals without ADHD, often in attempts to enhance cognitive performance. Some studies have investigated its effects in sleep-deprived and non-sleep-deprived healthy individuals. While animal research has shown promising results, the evidence in healthy humans is mixed and inconsistent. This has raised concerns about potential misuse, dependence, and the ethical implications of using prescription stimulants for performance enhancement.
It’s important to note that while Ritalin and generic methylphenidate share the same active compound, they may differ slightly in formulation, release mechanism (e.g., immediate vs. extended release), and how individuals respond to them. Generics are typically more cost-effective, while brand names like Ritalin may be preferred in certain clinical situations.

Methylphenidate: Clinical Potential and Pharmacological Profile [2-3]
Methylphenidate, a stimulant derived from the piperidine family, exists in four distinct stereoisomeric forms due to its two chiral centers. However, only specific isomers exhibit clinically meaningful central nervous system activity. Modern pharmaceutical formulations now exclude the inactive erythro isomers, focusing on the more effective enantiomeric pair.
Following oral administration, methylphenidate is rapidly absorbed, with peak plasma concentrations typically reached within 1 to 3 hours. Its bioavailability appears to improve when taken with food. The drug has a relatively short plasma half-life, around 1.5 to 2.5 hours, and minimal plasma protein binding, contributing to its fast clearance. Metabolism primarily occurs via hydrolysis to an inactive compound, ritalinic acid.
Beyond its core indications, including ADHD and narcolepsy, methylphenidate has been studied for potential use in a range of clinical scenarios. These include neurological recovery after brain injury or stroke, management of depressive symptoms in medically ill older adults, cancer-related fatigue, and support during ventilator weaning protocols. While not FDA-approved for these conditions, preliminary research suggests possible therapeutic benefits.
Approved for patients over six years of age, methylphenidate requires careful dose management due to risks such as appetite suppression and potential growth concerns in children. While these side effects are generally manageable, they underscore the importance of long-term monitoring, especially during developmental years. Additionally, concerns remain regarding its potential for misuse and dependency, particularly among individuals using it without medical supervision.
Overall, methylphenidate’s pharmacological profile continues to attract interest beyond traditional applications, particularly as research explores its role in enhancing motivation, mood, and cognitive function in diverse patient populations.
Treatment approaches for Attention Deficit Hyperactivity Disorder vary depending on individual needs, and methylphenidate remains one of the most established pharmacological options. First approved by the Food and Drug Administration in 1955, methylphenidate is now available in multiple formulations with distinct release mechanisms, such as immediate-release, extended-release, and osmotic-controlled oral system formulations. These formulations allow clinicians to tailor treatment based on age, symptom severity, and daily functioning. For example, United States guidelines recommend a maximum daily dose of 54 milligrams for the osmotic-controlled oral system and 60 milligrams for other formulations in children aged 6 to 12 years. International dosing protocols may differ, reflecting regional treatment guidelines and healthcare practices.

Learn ADHD medications: Methylphenidate Stimulants (Different ADHD medication with Methylphenidate). Methylphenidate vs Ritalin
Despite its widespread use and high efficacy in improving core Attention Deficit Hyperactivity Disorder symptoms, approximately 30% of patients either do not respond adequately to methylphenidate or experience side effects such as insomnia, dizziness, or appetite suppression. For these individuals, alternative pharmacological treatments include other stimulants (like amphetamines) and non-stimulants, such as bupropion, guanfacine, or atomoxetine. In addition, multimodal approaches that incorporate behavioral therapy, psychoeducation, parent training, or dietary interventions (for example, omega-3 fatty acids) are widely recommended by international guidelines, including those from the National Institute for Health and Care Excellence and the British Association for Psychopharmacology.
In terms of its impact on brain function, methylphenidate appears to contribute to both structural and functional changes. Neuroimaging research in Attention Deficit Hyperactivity Disorder patients has shown that treatment may enhance or normalize volumes in specific brain regions such as the prefrontal cortex, cerebellum, and basal ganglia. Functional improvements in brain activity have also been observed in areas like the anterior cingulate cortex and striatum—regions involved in attention, cognitive control, and motor regulation.
At the cellular level, animal studies have shown that methylphenidate can influence neuroplasticity by modulating neuronal firing, synaptic transmission, and even cellular differentiation, particularly in the hippocampus and prefrontal cortex. Chronic low-dose administration has been linked to increased neuronal proliferation, while higher doses seem to favor differentiation over cell growth. However, the translation of these findings to clinical settings remains limited, as dosing and administration routes in animal models often do not reflect human pharmacological conditions.
Although the classic mechanism of methylphenidate involves inhibition of dopamine and norepinephrine reuptake, recent studies suggest additional pathways may contribute to its effects. These include potential interactions with glutamatergic and serotonergic systems, as well as intracellular processes like vesicular monoamine transport mediated by vesicular monoamine transporter 2 and Wnt signaling pathways. The drug’s ability to improve attention and reduce hyperactivity—often referred to as its “paradoxical effect”—continues to be a subject of research, particularly given that such calming outcomes are not typical of psychostimulants in non-Attention Deficit Hyperactivity Disorder populations.
Furthermore, questions remain regarding the long-term neurological consequences of methylphenidate use, especially in developing brains. While short-term efficacy and safety are well-documented, longitudinal studies on developmental impact, receptor density changes, and sustained cognitive effects are still ongoing. Ethical limitations on pediatric neuroimaging complicate this area of research, emphasizing the need for innovative, non-invasive methods to assess the full scope of methylphenidate’s long-term action.
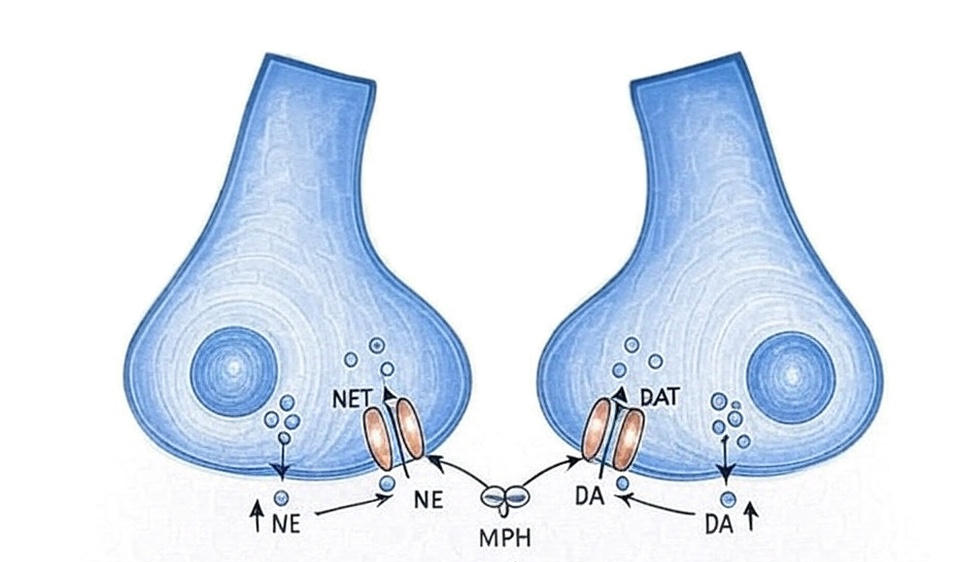
Figure 2 Mechanism of action of Metgilphenidat. Methylphenidate vs Ritalin
Additional Research on Methylphenidate vs Ritalin and Their Side Effects [4]
Ritalin and methylphenidate are both central nervous system stimulants widely used to treat Attention Deficit Hyperactivity Disorder (ADHD). Ritalin is the brand-name version of methylphenidate, and both medications work by increasing dopamine and norepinephrine levels in the brain to improve focus and reduce impulsivity.
In terms of effectiveness, Ritalin has been shown to help about 80% of patients with ADHD, with effects typically starting within 30 to 60 minutes. Generic methylphenidate offers similar benefits, though its effects may last longer—usually 4 to 6 hours. The best option varies depending on individual response, weight, and other health factors, so treatment should be personalized under medical guidance.
Regarding safety, both drugs share similar side effects such as nausea, headaches, and insomnia. Ritalin may cause anxiety and increased heart rate, while methylphenidate can more commonly lead to stomach discomfort. Long-term use of Ritalin is generally safe when properly managed, but methylphenidate may carry a slightly higher risk of dependence if misused.
Ultimately, the choice between Ritalin and methylphenidate should be made with a healthcare professional, taking into account the patient’s medical history, treatment goals, and possible side effects to find the most effective and safest approach.
Side Effects of Ritalin vs Methylphenidate
When treating attention deficit hyperactivity disorder (ADHD), both Ritalin and Methylphenidate are central nervous system stimulants that increase dopamine and norepinephrine levels in the brain. Understanding their potential side effects is important for making an informed choice.

Taking Ritalin For The First Time! What It Feels Like. Methylphenidate vs Ritalin
Common Side Effects
Both medications share similar side effect profiles, though some differences exist. Ritalin commonly causes nausea, headaches, dizziness, and insomnia. Methylphenidate often leads to stomach upset, anxiety, mood changes, and sleep disturbances
Differences in Side Effects and Onset
Ritalin acts quickly, usually within 30 minutes to an hour, which can influence the type and intensity of side effects experienced. Methylphenidate has a slower onset but a longer duration, which may alter how side effects manifest. For instance, some patients report more stomach upset and anxiety with Ritalin, while headaches and dizziness might be more frequent with Methylphenidate.
Long-Term Side Effects
Long-term use of either drug can lead to more serious effects. Ritalin may increase the risk of dependence, elevated heart rate, blood pressure, and ongoing sleep problems. Methylphenidate’s long-term effects can include mood swings, depression, anxiety, and appetite suppression.
Experience Report. Methylphenidate vs Ritalin [6-7]

Figure 3 Snorting. Methylphenidate vs Ritalin
Snorting Crushed Methylphenidate for Focus. Methylphenidate vs Ritalin
Setting: Alone at night, working at my desk on the computer.
Background: Took 36 mg extended-release methylphenidate (Concerta) 14 hours earlier, daily 0.2 mg clonidine for insomnia, and used a nicotine vape intermittently.
Timeline:
- T-21:40: Snorted 1/4 lines of crushed Concerta; nasal congestion required splitting doses.
- T-21:50: Effects begin, slight stimulation, working faster catching up on bookkeeping. Snorted 2nd line.
- T-22:00: Stronger effects; mood lifted from prior frustration. Headache briefly distracts. Snorted 3rd line.
- T-22:10: Working extremely fast; unusually strong focus and motivation. Finished dosing (45 mg total). Took clonidine but still wide awake.
- T-22:25: Distracted by texts, feeling motivated about work (rare). Noticed leg shaking.
- T-22:40: Effects slightly waning but still present. Considered redosing but decided against due to early morning. Noted nasal discomfort and challenging pill preparation.
- T-22:45: Sweaty hands, cognitive euphoria kicks in after vaping. Noticed hand tremors.
- T-22:50: Mixed feelings about working memory, runny nose due to recent illness, slight lightness in limbs.
- T-23:05: Effects fading somewhat; feeling a form of cognitive fatigue. Work productivity remains high — about 3x normal output. Compared effect duration to cocaine, noting methylphenidate lasts longer and lacks distracting euphoria.
- T-23:15: Reflected on effects in non-ADHD users, experienced typical dry mouth, rapid and connected thoughts, unusual writing productivity. No signs of peak fading, feeling alert again.
- T-23:30: Clearly coming down; no harsh crash, mild head tension, clonidine sedative effects overridden by methylphenidate. Noted this was the strongest insufflated experience despite prior higher doses. Recognized methylphenidate’s value beyond “poor man’s cocaine.”
- T-00:00: Effects similar to 30 minutes prior, more sober but still motivated. Strong desire to continue working but opted against more dosing to avoid sleep loss.
- T-00:30: Fully coming down, feeling sleepy. Concluded methylphenidate is an effective focus aid; plans to use insufflation again for work productivity.

Ritalin Snorting Experience at the Fair: A Cautionary Tale
It was a Saturday night during the fair in my town. I bought 2 crushed 20mg Ritalin tablets from a friend in exchange for tickets and decided to try snorting them behind some bleachers near the carnival trailers. Rolling a $5 bill, I snorted both tablets. At first, it was surprisingly easy on my nose—but that was the last good feeling.
Timeline:
- 6:30 PM: Snorted 40 mg of crushed Ritalin.
- 7:00 PM: Felt quick, jittery, and oddly happy.
- 8:00 PM: Effects began fading; body felt heavy and sluggish.
- 9:00 PM: Full comedown hit; I felt awful.
- 11:30 PM: My ride arrived; I struggled to look normal while saying goodnight to my mom.
- 11:45 PM: Tried to sleep but failed, watching swirling colors behind my closed eyes, replaying memories of the fair.
- 1:00 AM: Smoked marijuana to help sleep, but ended up lying awake for three hours.
- 4:24 AM: Still wide awake, mouth dry and gross despite brushing teeth, barely able to keep fluids down; eating was impossible.
Throughout, I felt jittery and spacy—wandering alone, even awkwardly offering to sell Ritalin to strangers. My stomach hurt, and my mouth was unbearably dry, forcing me to suck on ice to cope since drinking made me gag. After a few hours, my body felt heavy and sluggish. The experience was miserable, with a long comedown leaving me drained and sleepless.

Conclusion
Methylphenidate and Ritalin share the same active compound and are effective treatments for ADHD, though they differ slightly in formulation, onset, and duration. Ritalin, a brand-name version, may act faster, while generic methylphenidate can last longer. Both increase dopamine and norepinephrine to improve focus and impulse control, with similar side effect profiles. Long-term use requires monitoring due to potential developmental effects and misuse risks. Treatment should be personalized to ensure safety and effectiveness.
Bibliography
- https://www.drugs.com/compare/methylphenidate-vs-ritalin
- Thomas D. Challman MD James J. Lipsky MD Methylphenidate: Its Pharmacology and Uses Mayo Clinic Proceedings
- Volume 75, Issue 7, July 2000, Pages 711-721 https://doi.org/10.4065/75.7.711 https://www.sciencedirect.com/science/article/abs/pii/S0025619611646181
- Yde Ohki, Cristine Marie. Involvement of the Wnt Signaling in Methylphenidate (Ritalin) Treatment of ADHD. 2024, University of Zurich, Faculty of Science https://doi.org/10.5167/uzh-259346 https://www.zora.uzh.ch/id/eprint/259346/
- https://meds.is/en/comparison/ritalin-vs-methylphenidate-oral
- https://psychonautwiki.org/wiki/Methylphenidate#Subjective_effects
- https://psychonautwiki.org/wiki/Experience:Methylphenidate_(45mg,_Insufflated)_-_Phenomenal_Focus_Aid
- https://www.erowid.org/experiences/exp.php?ID=17503
- https://www.erowid.org/experiences/subs/exp_Pharms_Methylphenidate.shtml
- https://bbgate.com/threads/psychedelic-therapy-perspective-2025.16095/