
Abstract
Nitrazepam: A Powerful Benzodiazepine Drug with Diverse Properties. Nitrazepam is a benzodiazepine drug known for its potent hypnotic effects, as well as its sedative, anxiolytic, amnestic, anticonvulsant, and skeletal muscle relaxant properties. It is commonly referred to as “moggies” in street lingo. Nitrazepam has been found to reduce the time needed to fall asleep and increase the duration of sleep. Some studies suggest a synergistic depressant effect when nitrazepam is combined with alcohol. Additionally, it has been utilized for managing myoclonic seizures. This article provides a comprehensive overview of Nitrazepam, including general information, physico-chemical properties, recreational pharmacology, effects and symptoms, street names, prices and approximate dosage, potential dangerous interactions, legal status, synthesis of 7-nitro-5-phenyl-1,3-dihydro-1,4-benzodiazepin-2-one, conclusion, and bibliography. By delving into these aspects, this article aims to shed light on the multifaceted nature of Nitrazepam as a benzodiazepine drug. Please note that it is crucial to use and discuss Nitrazepam and other benzodiazepine drugs only under the guidance and prescription of a qualified healthcare professional.
General Information About Nitrazepam [1-4]
Other synonyms names of Nitrazepam are: Benzalin; Neozepam; Imeson; Mogadon; Neuchlonic; Calsmin; Calsamin; Eunoctin; Eunoktin; Imesont; Radedorm; Sonebon; Trazenin; Hipnax; Hipsal; Nelmat; Surem; Epibenzalin; Epinelbon; Nitrenpax; Nitrempax; Somitran; Sonnolin; Unisomnia; Dumolid; Nelbon; Paxisyn; Pelson; Relact; N-Desmethylnimetazepam; Persopit; Gerson; Ibrovek; Eatan; Dormin-5; Nitrazepamum; Magadon; Megadon; Mogadan; S 2000; Dormo-Puren; Mitidin; Eatan N; 2,3-Dihydro-7-nitro-5-phenyl-1H-1,4-benzodiazepin-2-on; Dormo-Puren; Ipersed; Nitravet; Noctesed; Pacisyn; Somnased; Somnibel.
IUPAC Name of Nitrazepam: 7-nitro-5-phenyl-1,3-dihydro-1,4-benzodiazepin-2-one
CAS numbers is 146-22-5
Trade names are Alodorm, Apodorm, Arem, Cerson, Insoma, Insomin, Mogadon, Nitrados, Nitrazadon, Nitrosun, Nitravet, Ormodon, Paxadorm, Remnos, Epam and Somnite.
Physico-Chemical Properties of Nitrazepam [1-4]
- Molecular Formula C15H11N3O3
- Molecular Weight 281.266
- Melting Point 223-227 °C; 225 °C (Decomposes)
- Solubility: >42.2 [ug/mL] (The mean of the results at pH 7.4)
- Color/Form: Solid
Structural formula of Nitrazepam present on Figure 1.
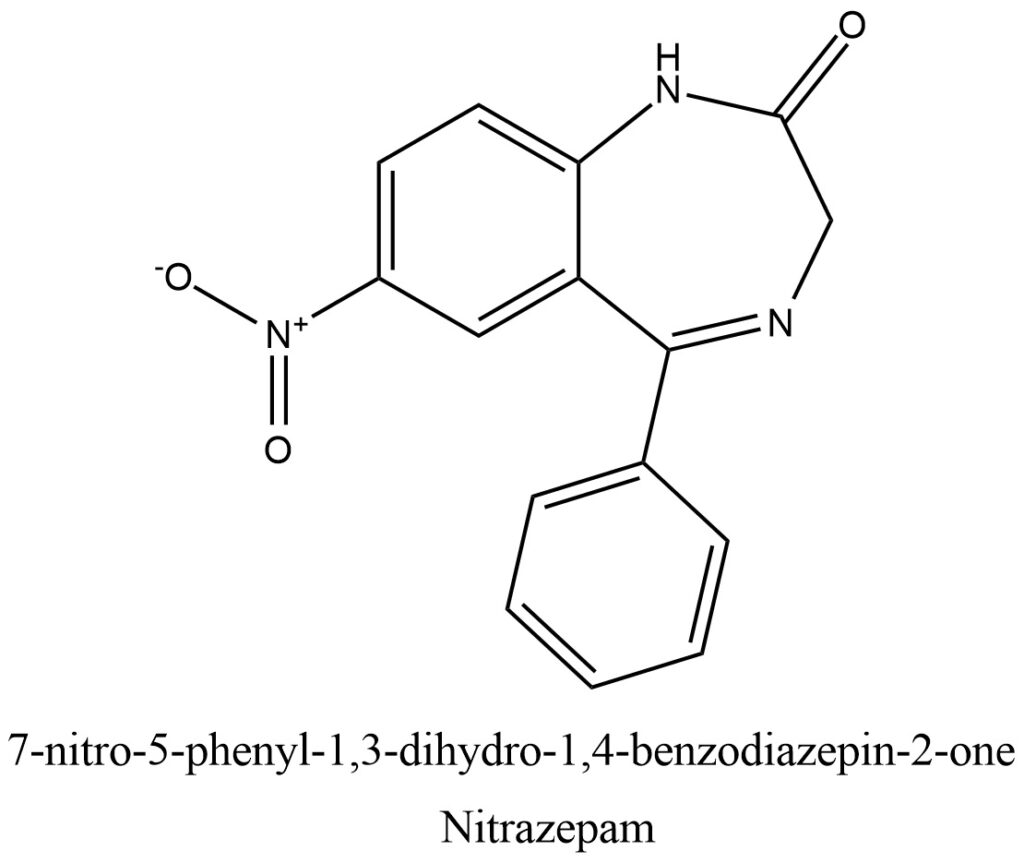
Figure 1. Structure of Nitrazepam
Commercial and crystalline solid possible of the Nitrazepam can be seen in the pictures provided in Figure 2 and Figure 3.

Figure 2. Commercial Nitrazepam
Figure 3. Crystalline solid of Nitrazepam
General Information of Nitrazepam in Recreational Use and Pharmacology [5, 6]
Nitrazepam (NZP) has been utilized in Europe since 1963 as a powerful sleep-inducing agent and an antiepileptic drug (AED). While it has been approved for use as an AED in Canada, it is not commercially available in the United States. Therapeutically, Nitrazepam falls into the categories of antiepileptic agent, hypnotic agent, and benzodiazepine derivative.
As a benzodiazepine, Nitrazepam acts on central benzodiazepine receptors that are associated with inhibitory GABA (gamma-aminobutyric acid) receptors, leading to enhanced GABA binding activity. GABA is a major neurotransmitter in the brain that promotes somnolence, muscle relaxation, and a decrease in anxiety, resulting in general central nervous system depression. Nitrazepam also possesses anticonvulsant properties, which may be attributed to its ability to bind to voltage-dependent sodium channels, limiting sustained repetitive firing by slowing the recovery of sodium channels from inactivation.
Nitrazepam is primarily used for short-term treatment of sleeping problems (insomnia), including difficulty falling asleep, frequent awakening, early awakening, or a combination of these issues. In some cases, Nitrazepam may be tried for epilepsy when other medications have failed, particularly in the treatment of West syndrome, an age-dependent epilepsy that affects young children. Uncontrolled studies have shown effectiveness of Nitrazepam in infantile spasms, but long-term use may lead to drowsiness, hypotonia, and tolerance to its antiepileptic effects, often limiting its use to acute seizure management.
Researchers have also developed a light-activated derivative of Nitrazepam called fulgazepam for experimental purposes. NZP is rapidly absorbed from the gastrointestinal tract, with peak blood concentrations occurring within 2 to 3 hours after oral administration. The plasma half-life ranges from 20 to 40 hours (average 26 hours), and while no specific therapeutic plasma level has been defined, toxic effects have been observed at plasma concentrations of 200 ng/ml. Some patients may develop tolerance to the antiepileptic properties of NZP, similar to what has been reported for clonazepam, although controlled studies on this topic are lacking.
Clinical Use
NZP is primarily indicated for the treatment of infantile spasms, myoclonic seizures, atonic seizures, and atypical absence seizures.
In numerous well-controlled studies, NZP has been used predominantly for the treatment of infantile spasms accompanied by hypsarrhythmia. Dreifuss et al. conducted a multicenter randomized study comparing the efficacy and safety of NZP and ACTH in 48 infants with infantile spasms. Both drugs exhibited similar efficacy during the 4-week treatment course. However, noteworthy adverse effects were observed in patients treated with ACTH, which were qualitatively more severe and necessitated treatment discontinuation in six patients. Therefore, the concomitant use of ACTH and NZP at the initiation of therapy is favored by the authors. Following a 10 to 15-day course, depending on the clinical response and improvement in serial EEG, ACTH is discontinued and NZP is continued as a long-term therapy. NZP has also shown effectiveness in myoclonic seizures in children and in the treatment of Lennox-Gastaut syndrome with atonic seizures and atypical absence seizures. As adjunct therapy, it may be effective for simple or complex partial seizures and most refractory seizure disorders. In our center, NZP is used as an adjunct to CBZ or PHT in any form of resistant partial epilepsy, with the majority of children tolerating this drug combination well. Overall, NZP has shown to produce fewer adverse effects in our experience compared to CZP, and tolerance to its antiepileptic effect appears to develop less rapidly than with CZP.
Neonatal Seizures
Neonatal seizures are a challenging condition to manage, and over the past 4 years, were have found NZP to be highly effective in controlling status epilepticus and resistant seizures in the neonatal period. When intravenous PB at an optimal therapeutic blood level fails to adequately control seizures, were prefer to add NZP orally via a gastric tube, starting with an initial dose of 0.5 mg/kg/day, instead of intravenous PHT. In Europe, CZP, which is available as an intravenous solution, has shown comparable results with a usual administered dose of 0.1 mg/kg/day.
Febrile Seizures
Febrile seizures are a common condition, and Vanasse et al. have discovered that NZP is an effective medication for preventing the recurrence of febrile seizures when used intermittently during episodes of fever. The effectiveness of NZP in this context is comparable to continuous treatment with PB, but without the adverse effects associated with long-term administration of PB.
Teratogeniclty
Research on the use of benzodiazepines during pregnancy has not shown evidence of teratogenicity. There have been cases where infants born to women treated with CZP showed transient apnea, cyanosis, and hypotonia, but no congenital malformations were observed. Cord blood levels of CZP were found to be within the therapeutic range. In a general review of prenatal exposure to benzodiazepines, particularly DZP, Grimm identified cases where transient adverse effects such as hypotonia at birth, apnea, hypothermia, and poor sucking were observed. Withdrawal symptoms in some cases included tremors, loose stools, vomiting, hyperactivity, and hypertonicity. In other patients, long-term effects such as learning disabilities and behavior problems resembling attention deficit syndrome have been reported.
Mortality [7]
The use of nitrazepam in the treatment of intractable epilepsy has been associated with an increased risk of death compared to other drug therapies. This risk may be higher in younger patients, specifically children below 3.4 years of age, with intractable epilepsy. However, in older children (above 3.4 years), the trend appears to be reversed in this study. Nitrazepam has been reported to potentially cause sudden death in children due to swallowing incoordination, high-peaked esophageal peristalsis, bronchospasm, delayed cricopharyngeal relaxation, and severe respiratory distress that may require ventilatory support. Nitrazepam may also contribute to the development of parasympathetic overactivity or vagotonia, leading to potentially fatal respiratory distress in children.
Hepatotoxicity
Nitrazepam, like other nitrobenzodiazepines, has been linked to severe hepatic disorders. Nitrobenzodiazepines, including nitrazepam, nimetazepam, flunitrazepam, and clonazepam, are known to be more hepatotoxic compared to other benzodiazepines. This increased hepatotoxicity is due to their metabolic activation by CYP3A4 enzyme, which can result in cytotoxic effects. The activation of these drugs can lead to the production of free radicals, oxidation of thiol, and covalent binding with endogenous macromolecules, ultimately resulting in oxidative damage to cellular components or inhibition of normal cellular function. The metabolism of a previously non-toxic drug into reactive metabolites has been linked to various adverse reactions.
Effects and symptoms of Nitrazepam Use [5, 6]
Adverse Effects
The primary adverse effects associated with NZP include sedation, lethargy, hypotonia, and ataxia. However, these adverse effects are typically temporary and tend to diminish after approximately 1 month of therapy. In infants, NZP may also cause drooling, eating difficulties, and aspiration pneumonia, which have been attributed to impaired swallowing due to crico-pharyngeal incoordination. There have been isolated reports of unexplained deaths in young children who received NZP at doses higher than 0.8 mg/kg/day. Additionally, some common side effects, occurring in at least 1% of individuals taking this medication, include those that can be managed or may resolve on their own over time.
- Clumsiness or unsteadiness;
- Dizziness;
- Drowsiness;
- Increased watering of mouth;
- Light headedness;
- Convulsions (seizures);
- Signs of a serious allergic reaction (i.e., abdominal cramps, difficulty breathing, nausea and vomiting, or swelling of the face and throat);
- Slow, weak, or shallow breathing;
- Symptoms of overdose (e.g., extreme sleepiness, confusion, slurred speech, slow reflexes, slow shallow breathing, loss of balance and coordination, uncontrolled eye rolling, low blood pressure, coma);
- Symptoms of withdrawal (e.g., feeling like you cannot move or respond, severe confusion, shivering, irregular heart rate and excessive sweating, feeling disconnected from reality, seeing or hearing things that aren’t there, believing things that aren’t true);
- Thoughts of self-harm or suicide.
- When taken improperly, the benzodiazepine medication nitrazepam, which is used to treat anxiety, sleeplessness, and alcohol withdrawal symptoms, can result in major health problems and even death.

Misuse of benzodiazepines among high-risk opioid users
Street Names, Prices and Approximate Dosage
Street names for Nitrazepam, also known as “moggies,” are commonly used among recreational users. Other general street names for benzodiazepines include “benzos,” “blues,” “valium,” and “vallies.” Less common street names include “fake vallies,” “street benzos,” “street blues,” “street valium,” and “street vallies,” as well as “Xanax,” “scoobies,” “scoobs,” “up-johns,” “whites,” and “yellows”.
The bioavailability of Nitrazepam ranges from 53% to 94% after oral administration. It is typically prescribed at a mean recommended dose of 0.25 to 1 mg/kg/day, with a maximum of 2 mg/kg/day, divided into three doses. Infants and small children may tolerate higher doses better. However, doses as low as 5 mg can impair driving skills.
Nitrazepam, when taken at doses of 5 mg or higher, can significantly impair vigilance performance and increase feelings of sleepiness. Like other hypnotic drugs, Nitrazepam is associated with an increased risk of traffic accidents. In the elderly, Nitrazepam has been linked to an increased risk of falls and hip fractures due to body balance impairments. The elimination half-life of Nitrazepam is 40 hours in the elderly and 29 hours in younger adults. To minimize adverse effects, it is recommended to initiate treatment with lower doses and gradually increase as tolerated and based on response. Dependence can develop in as little as four weeks, and tolerance to Nitrazepam’s effects often occurs with regular use. Changes in GABA levels in cerebral tissue and alterations in the serotoninergic system have been observed with Nitrazepam tolerance. Tolerance to the sleep-inducing and anticonvulsant effects of Nitrazepam can occur after approximately seven days. Withdrawal from Nitrazepam can result in symptoms similar to those seen with alcohol and barbiturates, including anxiety, insomnia, concentration problems, and fatigue. Discontinuation of short-term, single nightly dose therapy with Nitrazepam may lead to rebound insomnia.
Dangerous interactions [8-14]
An overdose of nitrazepam can result in impaired breathing, dizziness, decreased cognitive function and balance, bluish nails and lips, slurred speech, and extreme drowsiness, among other symptoms. In severe cases, these symptoms may progress to coma and even death.
Research findings suggest that there may be an increased association of nitrazepam molecules in the presence of alcohol, indicating a possible synergistic depressant effect when nitrazepam is combined with alcohol.
It is important to avoid using nitrazepam in patients with chronic obstructive pulmonary disease (COPD), particularly during acute exacerbations, as it may cause serious respiratory depression in those receiving hypnotics.
One case report described repetitive hallucinations and abnormal bodily sensations in a patient who received nitrazepam, triazolam, and subsequently erythromycin. Co-administration of benzodiazepine drugs at therapeutic doses with erythromycin may result in serious psychotic symptoms, particularly in individuals with other significant health complications.
Oral contraceptive pills have been shown to reduce the clearance of nitrazepam, potentially leading to increased levels of nitrazepam in the blood and accumulation. Rifampin, on the other hand, significantly increases the clearance of nitrazepam, while probenecid decreases its clearance. Cimetidine slows down the elimination rate of nitrazepam, resulting in prolonged effects and increased risk of accumulation. Combining alcohol with nitrazepam may result in a synergistic enhancement of the hypotensive properties of both benzodiazepines and alcohol. In animal experiments, benzodiazepines, including nitrazepam, have been shown to inhibit the glucuronidation of morphine, leading to increased levels and prolonged effects of morphine.
Legal Status
The legal status of nitrazepam varies by country. In Australia, it is classified as Schedule 4, which means it can only be obtained with a prescription. In Canada, it is categorized as Schedule IV, indicating that it is a prescription-only medication. In Germany, nitrazepam is also prescription-only, but higher doses are classified under Anlage III. On the international level, nitrazepam is listed as a Schedule IV psychotropic substance, indicating its controlled status.
Synthesis of 7-nitro-5-phenyl-1,3-dihydro-1,4-benzodiazepin-2-one [15]
The amide is formed by reacting 2-amino-5-nitrobenzophenone with bromoacetyl bromide. Nitrazepam is obtained through ring closure in liquid ammonia. Alternatively, diazepinone can be nitrated directly at the more reactive C7 position using potassium nitrate in sulfuric acid. Refer to Figure 4 for a visual representation.
Figure 4. General scheme of 7-nitro-5-phenyl-1,3-dihydro-1,4-benzodiazepin-2-one synthesis

Nitrazepam synthesis
Conclusion
It is imperative to follow your doctor’s instructions and take this medication exactly as prescribed. Avoid using larger doses or taking it for a longer duration than directed. If you miss a dose, take it as soon as you remember and resume your regular dosing schedule thereafter. If you are using Nitrazepam to help you sleep, refrain from taking it if it will prevent you from getting a full night’s rest (approximately 8 hours or more). Patients may feel confused, clumsy, and have difficulty focusing until the effects of the drug wear off. If you miss a dose during the day, skip it and continue with your regular dosing regimen. Do not double the dose.
The impact of age on the incidence of unintended CNS depression was most notable at high doses. Among over 80 individuals receiving an average daily dose of 10 mg or more of Nitrazepam, 55% reported undesired CNS depression. Elderly individuals may safely take low doses of nitrazepam, but high doses can cause severe CNS depression. The results suggest that, especially for elderly patients, there is minimal need to prescribe Nitrazepam at doses exceeding 5 mg. Some studies suggest a synergistic depressant effect when nitrazepam is used in combination with alcohol.
Bibliography
- https://en.wikipedia.org/wiki/Nitrazepam#Synthesis
- https://pubchem.ncbi.nlm.nih.gov/compound/4506
- https://go.drugbank.com/drugs/DB01595
- https://www.chemspider.com/Chemical-Structure.4350.html
- The Medical Treatment of Epilepsy. 1st Edition. Edited ByStanley R. Resor, Henn Kutt. CRC Press, 1991, 760 p. https://doi.org/10.1201/9781003066736 https://www.taylorfrancis.com/books/edit/10.1201/9781003066736/medical-treatment-epilepsy-stanley-resor-henn-kutt?refId=fcae5de1-7d8a-41e4-a1d8-22193d5ac682&context=ubx
- Mahesh Hanmant Mohite, Vaishnavi Suresh Jadhav etc. Adverse Effects of Nitrazepam. IJARSCT, 2023, Volume 3, Issue 2, pp. 352-354. DOI: 10.48175/IJARSCT-7986 https://ijarsct.co.in/jan3i2.html
- Pertti J. Rintahaka, Jo Anne Nakagawa etc. Incidence of Death in Patients with Intractable Epilepsy During Nitrazepam Treatment. Epilepsia, 1999, 40, 1, pp. 492-496. https://doi.org/10.1111/j.1528-1157.1999.tb00746.x https://onlinelibrary.wiley.com/doi/10.1111/j.1528-1157.1999.tb00746.x
- Chandra Kant Bhardwaj, Suraj Prakash etc. Study of nitrazepam interaction with alcohol: an ultrasonic and physiochemical investigation. Canadian Journal of Chemistry, 2021, Volume 99, Number 12. https://doi.org/10.1139/cjc-2021-0042 https://cdnsciencepub.com/doi/full/10.1139/cjc-2021-0042
- NOBORU TOKINAGA, TSUYOSHI KONDO etc. Hallucinations after a therapeutic dose of benzodiazepine hypnotics with co-administration of erythromycin. Psychiatry and Clinical Neurosciences, 1996, 50, pp. 337-339. https://doi.org/10.1111/j.1440-1819.1996.tb00577.x https://onlinelibrary.wiley.com/doi/10.1111/j.1440-1819.1996.tb00577.x
- David J. Back, Michael L’E. Orme Pharmacokinetic Drug Interactions with Oral Contraceptives. Clinical Pharmacokinetics, 1990, volume 18, pp. 472–484. https://doi.org/10.2165/00003088-199018060-00004 https://link.springer.com/article/10.2165/00003088-199018060-00004
- Brockmeyer NH, Mertins L, Klimek K, Goos M, Ohnhaus EE Comparative effects of rifampin and/or probenecid on the pharmacokinetics of temazepam and nitrazepam. International Journal of Clinical Pharmacology, Therapy, and Toxicology, 1990, 28, 9, pp. 387-393. https://europepmc.org/article/med/2228325
- Hermann R Ochs MD, David J Greenblatt MD etc. Cimetidine impairs nitrazepam clearance. Clin. Pharmacol. Ther., 1983, Volume 34, Issue 2, pp. 227-230. https://doi.org/10.1038/clpt.1983.157 https://ascpt.onlinelibrary.wiley.com/doi/abs/10.1038/clpt.1983.157
- Barry S. Levine, SARAH KERRIGAN Principles of Forensic Toxicology. Springer Cham. 2020, 691 p. https://doi.org/10.1007/978-3-030-42917-1 https://link.springer.com/book/10.1007/978-3-030-42917-1#toc
- Gian-Maria Pacifici, Lars L. Gustafsson Metabolic Interaction between Morphine and Various Benzodiazepines. Acta pharmacol. et toxicol., 1986, 58, pp. 249-252. https://doi.org/10.1111/j.1600-0773.1986.tb00103.x https://onlinelibrary.wiley.com/doi/10.1111/j.1600-0773.1986.tb00103.x
- L. H. Sternbach, R. Ian Fryer etc. Quinazolines and 1,4-Benzodiazepines. X.1 Nitro-Substituted 5-Phenyl-1,4-benzodiazepine Derivatives. J. Med. Chem., 1963, 6, 3, pp. 261–265. https://doi.org/10.1021/jm00339a010 https://pubs.acs.org/doi/abs/10.1021/jm00339a010