

- The process of creating a drug - May 23, 2023
- How do scientists model mental disorders in animals? - May 23, 2023
Introduction
Delving into the realm of ketamine, a powerful compound that has garnered significant attention in the medical field, provides valuable insights. This article explores the chemical properties, synthesis methods, effects on the brain and body, safe usage and dosage guidelines, anesthesia applications, and the legal status and ethical considerations associated with ketamine. By examining these facets, we can gain a comprehensive understanding of this remarkable substance and its multifaceted nature.

Ketamine Chemical and Physical Properties
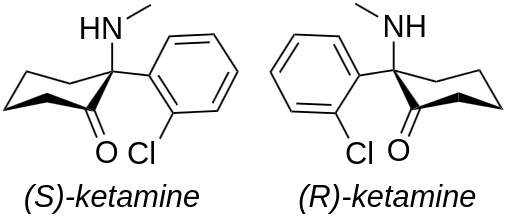
Ketamine, also known as (RS)-2-(2-Chlorophenyl)-2-(methylamino)cyclohexanone, is categorized as one of the arylcyclohexylamine compounds, which are synthetic organic substances. These compounds, called arylcyclohexylamines, derive their name from their chemical structures, which consist of an aromatic ring attached to a cyclohexane ring along with an amine group. It has molecular formula being C13H16ClNO. It is classified as a chiral molecule due to the presence of an asymmetric carbon atom, resulting in two enantiomers: (S)-ketamine and (R)-ketamine. The molecular weight of ketamine is approximately 237.7 g/mole.
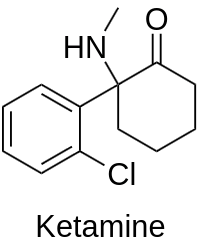
The chemical structure comprises a cyclohexane ring substituted with an -Oxo group (cyclohexanone), and a phenyl ring with a chlorine substituent at R2. Additionally, an amino methyl chain (-N-CH3) is connected to the same position (R1) of the cyclohexanone ring.
Physically, ketamine typically presents itself as a white crystalline powder or as a clear liquid when in its pharmaceutical solution form. It possesses a moderate to high solubility in water, allowing for ease of administration via various routes such as intravenous, intramuscular, or oral.
Furthermore, ketamine has a relatively high lipophilicity, enabling it to readily cross the blood-brain barrier and exert its psychoactive effects. This property contributes to its rapid onset of action, making it a valuable tool for anesthesia induction and other medical applications.
- CAS Number: 6740-88-1
- Trade names: Ketalar, others
- Street names: “Special K”, “K”, “Kit Kat”, “kitty”, and “horse/dog/cat tranquilizer” (which refers to its use in veterinary medicine), “Cat Valium”, and “Jet”
- Other names: CI-581; CL-369; CM-52372-2
- Melting point: 92°C (198 °F)
Ketamine Enantiomers
Ketamine consists of an equal mixture of two enantiomers, namely esketamine and arketamine.
When compared to norketamine, esketamine exhibits a greater potency as an NMDA receptor antagonist and as a dissociative hallucinogen. Based on the hypothesis suggesting that the antidepressant effects of ketamine stem from NMDA receptor antagonism, esketamine was specifically developed as an antidepressant.
Nonetheless, various other NMDA receptor antagonists, including memantine, lanicemine, rislenemdaz, rapastinel, and 4-chlorokynurenine, have thus far not demonstrated sufficient effectiveness in the treatment of depression.
Additionally, findings from animal studies suggest that arketamine, the enantiomer with a comparatively weaker NMDA receptor antagonism, and (2R,6R)-hydroxynorketamine, a metabolite that exhibits minimal affinity for the NMDA receptor but acts as a potent alpha-7 nicotinic receptor antagonist, may possess antidepressant properties.
Ketamine Synthesis
In laboratory-scale synthesis, there are two approaches available. The initial method involves the reaction between cyclopentyl Grignard and o-chlorobenzonitrile. This reaction produces o-chlorophenyl-cyclopentyl ketone. Subsequently, the ketone undergoes alpha bromination, followed by a reaction with methylamine to yield an alpha-hydroxy imine known as 1-Hydroxycyclopentyl-(o-chlorophenyl)-ketone-N-methylimine. When this imine is heated, a unique alpha-hydroxyimino rearrangement occurs, resulting in the formation of Ketamine. The overall yield for this synthesis is approximately 60%.

In the second approach, the conversion of compound (1) was achieved through its reaction with methylamine. The reaction took place under dark and solvent-free conditions, in the presence of 0.04 g of potassium carbonate. Subsequently, compound (2) underwent a thermal rearrangement resulting in the production of ketamine (3). For this rearrangement step, two different high boiling point solvents, namely decaline and diphenyl ether, were employed. The findings indicated that when the rearrangement was conducted in diphenyl ether, the yield of this step reached 50%. However, the utilization of decaline as a solvent in this particular step enhanced the yield significantly, yielding a higher efficiency of 72.5%. Consequently, decaline was selected as the solvent for the rearrangement step, and the temperature was elevated to the reflux temperature of decaline (170 °C) to achieve the optimal outcome.

Ketamine Pharmacology Effects: How It Influences the Brain and Body
Ketamine is categorized as a non-competitive antagonist of the NMDA receptor. The NMDA receptor, which is an ionotropic glutamate receptor, facilitates the transmission of electrical signals between neurons in the brain and spinal cord. For these signals to propagate, the receptor must remain open. Dissociative substances work by closing the NMDA receptors through blockade. This disruption of neuronal connectivity results in a loss of sensation, impaired movement, and ultimately, the characteristic state known as the “K-hole.”
Ketamine is among the most well-known dissociative compounds, belonging to a diverse group that includes phencyclidine (PCP), methoxetamine (MXE), dextromethorphan (DXM), and nitrous oxide.

In high doses, reaching a fully anesthetic level, ketamine has been observed to bind to μ-opioid receptors type 2 in cultured human neuroblastoma cells, albeit without demonstrating agonist activity. Additionally, it interacts with sigma receptors in rats. Ketamine also affects muscarinic receptors, descending monoaminergic pain pathways, and voltage-gated calcium channels.
At subanesthetic and fully anesthetic doses, ketamine has been found to hinder serotonin depletion in the brain by inhibiting 5-HT receptors, rather than through the inhibition of monoamine oxidase.
The estimated bioavailabilities for ketamine are as follows: nasal administration (45%), oral ingestion (17%), and rectal administration (25%).
Physical effects:
- Sedation: Ketamine is known to induce a moderate sedating effect, discouraging physical activity and potentially immobilizing the user at higher doses.
- Spontaneous bodily sensations: The “body high” experienced with ketamine can be described as a sharp, pleasurable, tingling sensation that is localized in the hands, feet, and head. This may result in an out-of-body experience or a sense of disconnection between the mind and body, accompanied by physical euphoria.
- Alterations in bodily perception and gravity perception: Ketamine can significantly modify how users perceive their bodily form, with the intensity varying depending on the dosage. At k-hole doses, individuals may feel completely disconnected from their body and the Earth.
- Physical euphoria: While some users may experience physical euphoria, it is not as strong or consistent as with opiates or MDMA.
- Sensation of bodily lightness: Users may perceive their body as floating and weightless, particularly at low doses. This effect can be oddly stimulating, making physical movement feel effortless.
- Loss of motor control: Ketamine commonly leads to a loss of gross and fine motor control, balance, and coordination, particularly at higher doses. It is recommended for users to be seated during the onset to prevent falls and injuries.
- Increased blood pressure: Higher doses of ketamine have been shown to cause increased blood pressure.
- Dehydration: There is a risk of minor to moderate dehydration, particularly in hot and physically demanding environments like dance floors.
- Tactile suppression: Ketamine can suppress the sense of touch, resulting in feelings of numbness in the extremities.
- Pain relief: Ketamine provides significant pain relief, as most physical sensations are suppressed while under its influence.
- Optical sliding: Users may experience involuntary eye movements, known as nystagmus, especially at higher doses. This effect is temporary and typically not a cause for concern unless it persists after other effects have subsided.
- Dizziness: Some users may report dizziness during ketamine intoxication.
- Increased salivation
- Nausea: Although uncommon, nausea is more likely to occur at higher doses and closer to the peak of the experience.
- Gustatory hallucination
- Difficulty urinating
- Decreased libido: Unlike stimulants and many other substances, ketamine tends to significantly decrease libido, making sexual activity unappealing and challenging. This effect aligns with tactile suppression and orgasm suppression.
- Orgasm suppression: Ketamine strongly inhibits orgasms and the normal sexual arousal response at moderate to high doses.
- Physical autonomy: While relatively uncommon, some users may experience a sensation of their body performing gestures and movements beyond their control. However, these disturbances are typically simple and short-lived.
Visual effects:
- The visual effects of ketamine are highly suppressive and distortive. It is crucial to never drive or operate machinery while under the influence of ketamine.
- Suppression:
- Double vision: Prominent at moderate to heavy doses, making it difficult to read text unless one eye is closed.
- Suppression of pattern recognition: Generally occurs at higher doses, leading to an inability to recognize and interpret visual information.
- Suppression of acuity
- Frame rate suppression: Dose-dependent and more noticeable at higher doses.
- Distortions:
- Perspective distortion
- Environmental cubism
- Environmental orbism
- Scenery slicing
- Geometry:
- The visual geometry induced by ketamine is characterized by vibrant colors compared to less visually disconnecting dissociatives like MXE and PCP. However, it is not as intricate as the geometric patterns experienced with DXM or traditional psychedelics.
- Ketamine-induced visual geometry typically ranges up to level 4 and can be described as simplistic in complexity, algorithmic in style, synthetic in appearance, unstructured in organization, dimly lit, multicolored, glossy in shading, soft-edged, large in size, fast in motion, smooth in movement, with a balance of rounded and angular corners, immersive in depth, and consistent in intensity.
- Hallucinatory states:
- Higher doses of ketamine can elicit a wide range of high-level hallucinatory experiences, although they are less consistent and reproducible compared to many common psychedelics. These effects include:
- Machinescapes
- Internal hallucination (autonomous entities, settings, sceneries, landscapes, perspective hallucinations, scenarios, and plots): These hallucinations can be described as delirious in believability, fixed in style, providing new experiences and memory replays in content, autonomous in controllability, and solid in style.
- External hallucination (autonomous entities, settings, sceneries, landscapes, perspective hallucinations, scenarios, and plots): These hallucinations can be described as delirious in believability, autonomous in controllability, and solid in style. The most common theme experienced with this effect is interacting and conversing with friends who are not actually present.
- Higher doses of ketamine can elicit a wide range of high-level hallucinatory experiences, although they are less consistent and reproducible compared to many common psychedelics. These effects include:
Cognitive effects:
- Analysis suppression: Users report difficulty in thinking normally or logically while under the influence of ketamine. Normal cognition and working memory are impaired in a dose-dependent manner. However, it is worth noting that creative or non-linear thinking abilities may become enhanced (referred to as conceptual thinking).
- Suppression of anxiety: Ketamine exhibits notable anxiety suppression at all doses, although it is not as selective as benzodiazepines or other GABAergics.
- Cognitive euphoria: Users report experiencing moderate to strong states of cognitive euphoria, primarily during the come-up phase. However, this effect appears to be less pronounced compared to stimulants, entactogens, and opioids.
- Compulsive redosing: Due to its euphoric effects, rapid onset, and short duration, ketamine can lead to compulsive redosing in some individuals. It is strongly recommended to employ strategies to limit intake and prevent abuse.
- Conceptual thinking: Ketamine induces conceptual or non-linear thinking, stimulating artistic or creative faculties. Users commonly describe entering dream-like, highly complex, and abstract mental states that transcend the boundaries of normal cognition, providing new insights into their lives and mental patterns.
- Déjà vu: Users may experience a powerful sensation of déjà vu, although this effect is less common compared to other substances.
- Delusion: Delusions are more likely to occur with ketamine use compared to other substances such as stimulants or psychedelics. This effect often coincides with ego inflation. Ketamine should be avoided by individuals susceptible to mental disorders like schizophrenia or bipolar disorder, as it may exacerbate delusions and trigger psychosis.
- Depersonalization and Derealization
- Reduction of depression symptoms
- Disinhibition: Low doses of ketamine can produce disinhibition similar to alcohol, making it occasionally used for this purpose at parties and raves. However, higher doses can result in social withdrawal and an inability to communicate effectively.
- Dream potentiation
- Ego inflation: Lower doses of ketamine may result in ego inflation, similar to the effects observed with alcohol, benzodiazepines, or cocaine. Ego inflation can also occur with k-hole doses, leading to delusions of grandeur.
- Suppression of focus: The ability to focus on a single task or object may be strongly suppressed. The mental effect of ketamine can be described as “scattering” and “non-linear” and occurs alongside analysis suppression.
- Enhancement of immersion: Ketamine significantly enhances the user’s sense of immersion, particularly when experiencing visual media. It is considered one of the most immersion-enhancing substances known.
- Increased appreciation of music: Ketamine may enhance one’s appreciation of music depending on the dose and setting. However, this effect is generally less consistent compared to psychedelics or entactogens. In some cases, ketamine may cause music to sound alien and unpleasant.
- Introspection: Some user reports suggest that ketamine may enhance introspection; however, this effect appears to be less consistent and robust compared to psychedelics and entactogens. It is important to note that there is limited evidence showing ketamine’s psychotherapeutic benefits.
- Memory suppression: Ketamine strongly suppresses short-term and long-term memory in a dose-dependent manner throughout the experience. Heavy doses can temporarily impair memory entirely, resulting in amnesia.
- Personal bias suppression: Some user reports suggest that ketamine may suppress personal bias; however, this effect appears to be less consistent and robust compared to psychedelics or entactogens.
- Mania
- Psychosis: Psychosis is more common with ketamine compared to other substances such as stimulants or psychedelics, often coinciding with the delusion effect. Ketamine should be avoided by individuals susceptible to mental disorders like schizophrenia or bipolar disorder, as it may exacerbate delusions and trigger psychosis.
- Spatial disorientation: Ketamine prominently affects spatial orientation in a dose-dependent manner. Users should carefully assess their surroundings while taking ketamine to avoid getting lost or causing injury.
- Enhancement of suggestibility: Ketamine may render the user significantly more suggestible during and after administration. This may be attributed to ketamine’s impact on cognition and susceptibility to delusions and psychosis.
- Thought deceleration: Users may perceive their thoughts as stiff, frozen, or in slow-motion. Dissociatives are known to produce this effect more strongly compared to other substances.
- Time distortion: Ketamine markedly alters the subjective experience of time, particularly at the k-hole threshold. Users may find it challenging to gauge the passage of time, with some reporting that it can feel like a lifetime within half an hour. Others describe being transported to a dimension seemingly beyond time and space until the effects wear off.
- Suppression of addiction: Ketamine is being actively studied as a potential treatment for alcohol use disorder, showing promising early results.
Auditory effects:
- Suppression of auditory perception
- Distortion of auditory sensations
- Auditory hallucinations
Disconnective effects: Ketamine is renowned for its disconnective effects, collectively known as “dissociation.” The following presents a breakdown of the various forms of sensory and mental disconnection commonly reported with ketamine use.
- Cognitive detachment
- Physical detachment
- Visual disconnection: This eventually leads to the experience of the infamous “k-hole” or, more specifically, gaps, voids, and spatial distortions alongside structures.
Multi-sensory effects:
- Synesthesia: Synesthesia is occasionally reported with ketamine, particularly at higher doses. Some users describe the ability to “hear colors” or “see sounds” while in the k-hole state. However, it remains unclear whether ketamine directly induces synesthesia as a typical effect or if it triggers it in predisposed individuals. Further research is necessary to understand the underlying causes of this reported effect.
Transpersonal effects: Transpersonal effects are sometimes reported with ketamine and other dissociatives. However, these effects appear to be less consistent and robust compared to those observed with psychedelics and entactogens.
It is important to note that there is currently limited clinical evidence supporting the psychotherapeutic benefits of ketamine, and some evidence suggests that it may contribute to disordered thinking.
- Existential self-realization
- Alteration of identity
- Near-death experiences
- Enhancement of spirituality
Safe Usage and Dosage of Ketamine
Ensuring the safe usage and proper dosage of ketamine is crucial to minimize risks and maximize its potential benefits. When it comes to medical applications, the dosage and administration of ketamine must be carefully determined by healthcare professionals based on individual patient characteristics, medical history, and the intended purpose of use.
For anesthesia induction, ketamine is typically administered intravenously at a dose of 1 to 2 milligrams per kilogram of body weight. This dosage may vary depending on factors such as the desired level of anesthesia, the patient’s age, and overall health condition. Close monitoring of vital signs and depth of anesthesia is essential during the procedure.
Ketamine dosage:
- Threshold – 5 mg
- Light 10 – 30 mg
- Common 30 – 75 mg
- Strong 75 – 150 mg
- Heavy 150 mg+
In the context of pain management and psychiatric applications, ketamine may be administered in lower doses through intravenous infusion or intramuscular injection. These doses are often referred to as sub-anesthetic or sub-psychedelic doses. The specific dosage can vary depending on the intended therapeutic purpose and the individual patient’s response.
It is important to note that ketamine should always be used under the supervision of trained healthcare professionals in a controlled environment. Adhering to proper medical protocols and guidelines is essential to minimize potential risks and adverse effects associated with its use.
Furthermore, ketamine should be used with caution in individuals with a history of substance abuse, cardiovascular conditions, or psychiatric disorders. Close monitoring and individualized assessment are necessary to ensure the suitability and safety of ketamine administration for each patient.
By following recommended dosages, closely monitoring patients, and considering individual factors, healthcare professionals can help optimize the safe usage of ketamine while minimizing potential risks and adverse effects.
Ketamine in Anesthesia
The utilization of ketamine in anesthesia reflects its unique characteristics. It is the preferred drug for short-term procedures where muscle relaxation is unnecessary. Ketamine’s impact on the respiratory and circulatory systems differs from other anesthetics. It minimally suppresses breathing compared to most available anesthetics. At anesthetic doses, ketamine typically stimulates rather than depresses the circulatory system. Essential airway reflexes remain intact, allowing for the administration of ketamine anesthesia without additional airway protection measures. However, the presence of psychotomimetic effects limits the acceptance of ketamine. Nevertheless, the use of lamotrigine and nimodipine can reduce these effects, and benzodiazepines or propofol can also counteract them.
Ketamine is frequently employed in the treatment of severely injured individuals and has shown to be safe in this population. It has been extensively used for emergency surgeries in field conditions, such as during the Vietnam War. A clinical practice guideline from 2011 supports the use of ketamine as a sedative in emergency medicine, particularly during physically painful procedures. Ketamine is the preferred choice for individuals in traumatic shock who are at risk of hypotension. For people with severe head injuries, low blood pressure poses a significant danger, and ketamine is unlikely to lower blood pressure. In fact, it often raises blood pressure, making it the most suitable option for those with severe head injuries.
Ketamine is also a viable option for children, either as the sole anesthetic for minor procedures or as an induction agent followed by a neuromuscular blocker and tracheal intubation. Specifically, children with cyanotic heart disease and neuromuscular disorders are ideal candidates for ketamine anesthesia.
Thanks to its bronchodilating properties, ketamine can be used for anesthesia in individuals with conditions such as asthma, chronic obstructive airway disease, and severe reactive airway disease, including active bronchospasm.
Ketamine Use Legal Status
Although ketamine is legally available for sale in numerous countries globally, it is classified as a controlled substance in several countries:
- Australia: Ketamine is a Schedule 8 drug in Australia, meaning that possession, manufacture or supply without authority is illegal.
- Austria: Ketamine is classed as a NR medication (prescription only, repeated dispense prohibited) and legal for medical and veterinary use, but illegal when sold, possessed or produced without a prescription under the NPSG (Neue-Psychoaktive-Substanzen-Gesetz).
- Belgium: Ketamine is legal for medical and veterinary use and illegal when sold or possessed without a prescription.
- Brazil: Ketamine is legal for veterinary use and illegal when sold or possessed for human use.
- Canada: Ketamine is controlled under Schedule I of the Controlled Drugs and Substances Act. Activities such as the sale, possession or production of ketamine are illegal unless authorized for medical, scientific or industrial purposes. In Canada, ketamine has legitimate uses in medicine.
- China: Ketamine is a Schedule II drug.
- Czech Republic: Ketamine is a Schedule IV (List 7) substance. Sold exclusively with a prescription “without a blue stripe” (§ 1, g), 1. of Nařízení vlády č. 463/2013 Sb.)
- Denmark: Ketamine is legal for medical and veterinary use and illegal when sold or possessed without a prescription.
- France: Ketamine is a Schedule IV drug in France.
- Germany: Ketamine is a prescription medicine, according to Anlage 1 AMVV.
- Hong Kong: Ketamine is a Schedule I drug in Hong Kong.
- Luxembourg: Ketamine is a prohibited substance for recreational use.
- Malaysia: Ketamine is illegal to sell and possess in Malaysia.
- Mexico: Ketamine is a Category 3 drug in Mexico.
- New Zealand: Ketamine is a Class C drug in New Zealand.
- Norway: Ketamine is a Class A drug in Norway.
- Singapore: Ketamine is a Class A drug in Singapore.
- Slovakia: Ketamine is a Schedule II drug in Slovakia.
- South Korea: Ketamine is illegal to possess and sell in South Korea.
- Spain: Ketamine is a Schedule IV drug in Spain.
- Sweden: Ketamine is a Schedule IV drug in Sweden.
- Switzerland: Ketamine is a controlled substance specifically named under Verzeichnis B, when possessed or handled without a license. Medicinal use is permitted.
- Taiwan: Ketamine is a Schedule III drug in Taiwan.
- Turkey: Ketamine is a ‘green prescription’ only substance and illegal when sold or possessed without a prescription.
- United Kingdom: Ketamine is a Class B drug in the United Kingdom.
- United States: Ketamine is a Schedule III drug in the United States.
- Poland: Ketamine is illegal to possess, manufacture and sell except for medical purposes.
Conclusion
In conclusion, exploring the science of ketamine enhances our understanding of its properties, effects, benefits, and synthesis. By delving into its chemical and physical characteristics, uncovering its effects on the brain and body, discussing safe usage and anesthesia applications, and addressing legal and ethical considerations, we gain a holistic perspective on ketamine’s multifaceted nature. Continued research and responsible use of ketamine hold promising prospects for its therapeutic potential in various medical domains.
Bibliography
- Sinner, B., and B. M. Graf. “Ketamine.” Modern anesthetics (2008): 313-333. https://link.springer.com/chapter/10.1007/978-3-540-74806-9_15
- Craven, R. “Ketamine.” Anaesthesia 62 (2007): 48-53. https://associationofanaesthetists-publications.onlinelibrary.wiley.com/doi/full/10.1111/j.1365-2044.2007.05298.x
- Morgan, Celia JA, H. Valerie Curran, and Independent Scientific Committee on Drugs (ISCD). “Ketamine use: a review.” Addiction 107.1 (2012): 27-38. https://onlinelibrary.wiley.com/doi/abs/10.1111/j.1360-0443.2011.03576.x
- Aan Het Rot, Marije, et al. “Ketamine for depression: where do we go from here?.” Biological psychiatry 72.7 (2012): 537-547. https://www.sciencedirect.com/science/article/abs/pii/S0006322312004179
- Gao, Mei, Damoon Rejaei, and Hong Liu. “Ketamine use in current clinical practice.” Acta Pharmacologica Sinica 37.7 (2016): 865-872. https://www.nature.com/articles/aps20165
- https://en.wikipedia.org/wiki/Ketamine
- https://psychonautwiki.org/wiki/Ketamine
- https://bbgate.com/threads/ketamine-synthesis.567
- https://bbgate.com/threads/ketamine-synthesis-from-2-2-chlorophenyl-2-hydroxycyclohexanone.1385
- https://erowid.org/chemicals/ketamine/