
- The process of creating a drug - May 23, 2023
- How do scientists model mental disorders in animals? - May 23, 2023
Abstract
Bupropion, also known by the brand name Wellbutrin, is a widely used aminoketone antidepressant primarily prescribed for major depressive disorder and smoking cessation. It is also commonly used as an add-on medication in cases where the first-line selective serotonin reuptake inhibitor (SSRI) antidepressant has an “incomplete response.” It should not be confused with Buprenorphine or Buspirone.
Unlike other antidepressants, Bupropion has several unique features, including its ability to improve symptoms of hypersomnia and fatigue without causing sexual dysfunction or weight gain. However, Bupropion therapy has been associated with transient, asymptomatic elevations in serum aminotransferase levels and rare instances of clinically apparent acute liver injury.
In summary, Bupropion is a highly effective medication for treating depression and supporting smoking cessation, with unique features that set it apart from other antidepressants. However, it is important to be aware of potential adverse effects and drug interactions before using this medication.
This article provides a comprehensive overview of Bupropion, covering its general information, physico-chemical properties, pharmacology in recreational use, effects and symptoms, toxicity and harm potential, street names, prices and approximate dosage, dangerous interactions, legal status, synthesis of 2-(tert-butylamino)-1-(3-chlorophenyl)propan-1-one, conclusion, and bibliography.
Bupropion: What You Need To Know
General Information About Bupropion [1, 2]
Other synonyms names of Bupropion are: Amfebutamone; Amfebutamon; amfebutamonum; Amfebutamona; (+-)-Bupropion; Elontril; Wellbatrin; Zyban; AMFEBUTAMONE HCl; alpha-(tert-butylamino)-m-chloropropiophenone
IUPAC Name of Bupropion: 2-(tert-butylamino)-1-(3-chlorophenyl)propan-1-one
CAS numbers are: 34911-55-2 (±)-Bupropion; 144445-76-1 (-)-Bupropion; 144445-75-0 (+)-Bupropion; 34841-39-9 BUPROPION
Trade names are Wellbutrin, Aplenzin, Budeprion, Buproban, Forfivo, Zyban, Bupron, Bupisure, Bupep, Smoquite, Elontril, Buxon.
Physico-Chemical Properties of Bupropion [1, 2, 3]
- Molecular Formula C13H18ClNO
- Molecular Weight 239.74
- Boiling point 334.8±27.0 °C at 760 mmHg; 52 °C at 0.005 mm Hg
- Melting Point 233-234 °C
- Solubility: In water, 140 mg/L at 25 °C (est); in methanol, ethanol, acetone, ether, benzene.
- Color/Form: pale yellow oil; powder with bitter taste
- Very hygroscopic and susceptible to decomposition
Structural formula of Bupropion present on Figure 1.
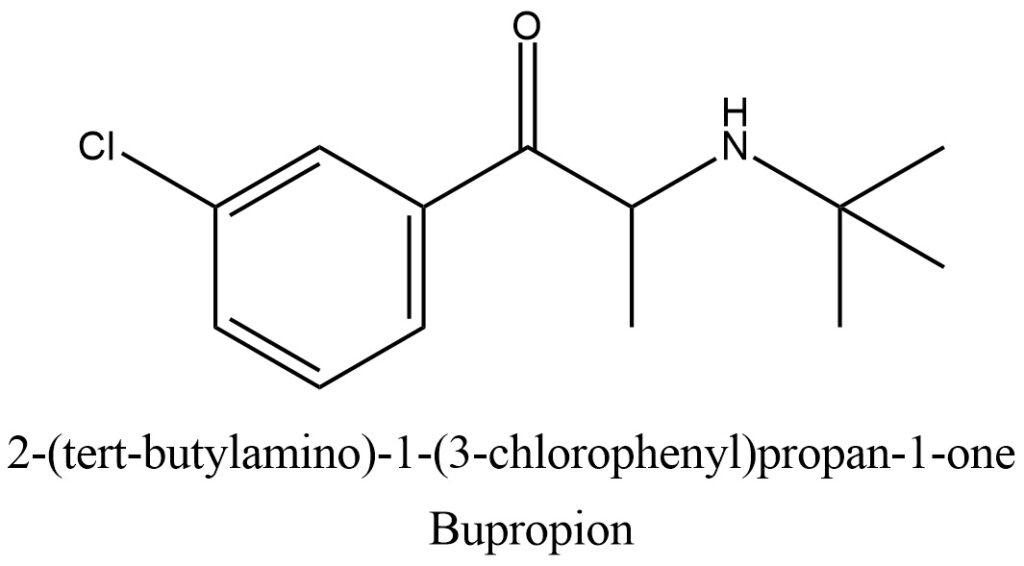
Figure 1. Structure of Bupropion
The Bupropion can be seen in the pictures provided in Figure 2 and Figure 3.

Figure 2. Commercial Bupropion

Figure 3. Pills of the Bupropion
General Information of Bupropion in Recreational Use and Pharmacology [1, 4-9]
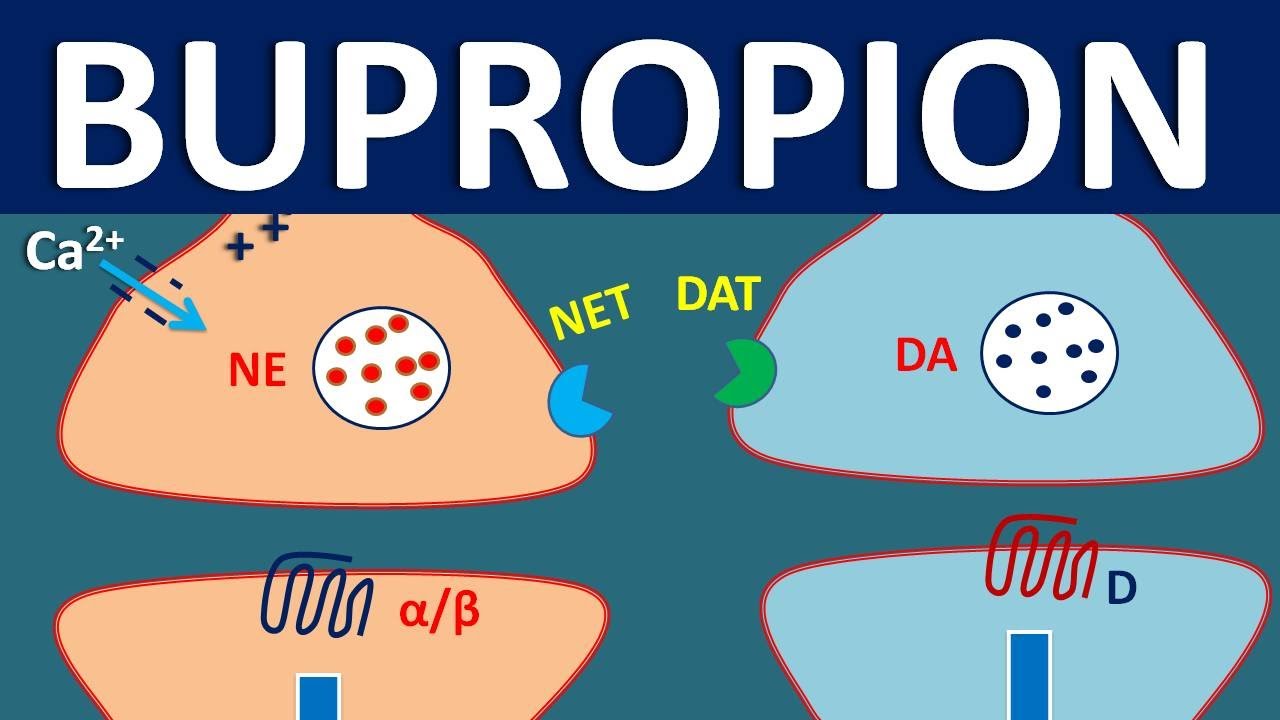
Bupropion, initially synthesized by Nariman Mehta of Burroughs Wellcome (now GlaxoSmithKline) in 1969, was granted a US patent in 1974. It was approved by the FDA as an antidepressant on December 30, 1985, and marketed under the name Wellbutrin. However, due to a high incidence of seizures at the recommended dose of 400-600 mg/day, the drug was withdrawn in 1986. Later, it was discovered that the risk of seizures was dose-dependent, and Bupropion was re-introduced to the market in 1989 with a lower maximum recommended daily dose of 450 mg/day. Unlike other known antidepressant agents, Bupropion has a unique chemical structure and does not inhibit monoamine oxidase or the serotonin transporter. Instead, Bupropion has a selective activity at dopamine and norepinephrine receptors, resulting in its CNS stimulant effects, making it a potential drug of abuse. Bupropion has also been found to have mild amphetamine-like activity, particularly when inhaled or injected. However, it can lower the seizure threshold and poses a risk of seizures when combined with other drugs or substances that lower the seizure threshold. Bupropion has also been shown to increase blood pressure and exacerbate pre-existing hypertension. In clinical trials, the mean increase in systolic blood pressure associated with Bupropion use was 1.3 mmHg, and it did not increase the incidence of CV events such as stroke or heart attack in smokers with CVD.
Effects and symptoms of Bupropion Use [4, 7]
Bupropion is notorious for causing highly unpleasant and potentially hazardous effects, especially when abused at high doses. Axsome Therapeutics, Inc. is currently developing a fixed-dose combination of dextromethorphan hydrobromide and bupropion hydrochloride (marketed as AUVELITYTM), which has been approved in the US in August 2022 for the treatment of major depressive disorder (MDD) in adults, as well as Alzheimer’s disease agitation and smoking cessation. Dextromethorphan is an uncompetitive N-methyl-D-aspartate (NMDA) receptor antagonist and sigma-1 receptor agonist, while bupropion is an aminoketone and CYP2D6 inhibitor that enhances the bioavailability of dextromethorphan.
Bupropion – Mechanism, side effects, precautions and uses
All effects in different categories [5]
ffects of Bupropion on Figure 4
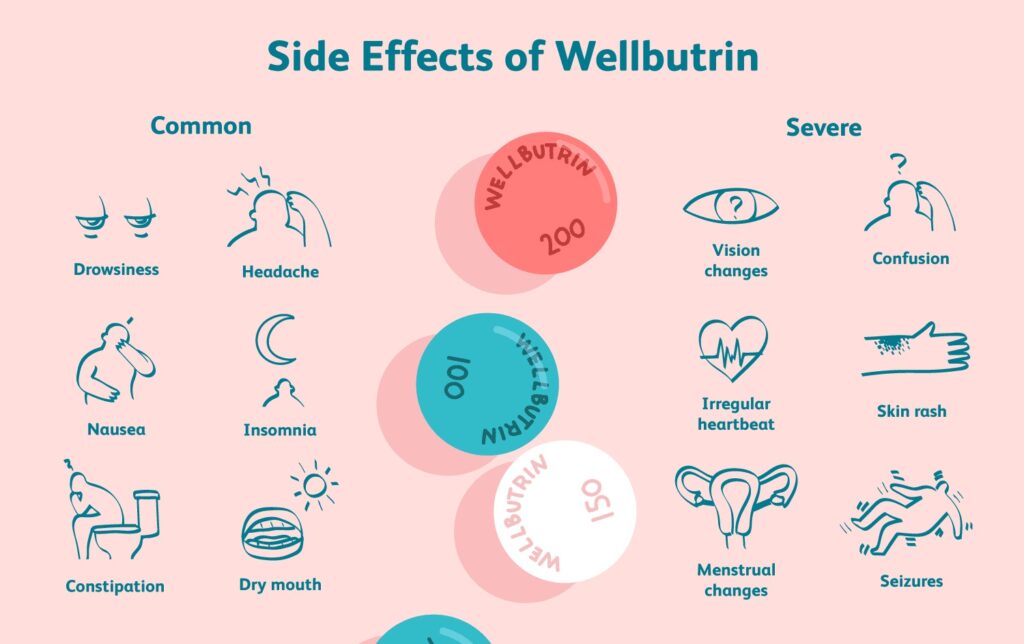
Figure 4. Effects of Bupropion
Physical effects:
- Stimulation – Bupropion’s NDRI activity makes it a stimulating substance.
- Spontaneous physical sensations – This effect is usually weak. It can be described as a mild and pleasant soft or sharp tingling sensation with warmth radiating from the body, according to other substances with similar pharmacology.
- Seizures – This effect becomes more likely proportional to dose.
- Increased heart rate
- Increased blood pressure
- Pupil dilation
- Appetite suppression
- Nausea
- Tactile hallucinations – This effect is usually only present at high doses.
- Temperature regulation suppression
Visual effects:
- External hallucinations
- Shadow people
- Drifting
- Pattern recognition enhancement
- Tracers
- Acuity suppression
Cognitive effects:
- Delirium – This occurs at high to very high and/or unreasonable doses and is a consequence of bupropion’s antagonism of nicotinic acetylcholine receptors (nAChRs). Unlike other deliriants, this effect can be very painful and hard to get away from because of bupropion’s ability to keep the user awake, unlike deliriants like diphenhydramine.
- Paranoia
- Disinhibition – This occurs mainly at recreational doses.
- Delusions – This effect is usually only present at very high doses.
- Anxiety – Bupropion causes more anxiety than other stimulants.
- Mania – Bupropion increases the risk of manic episodes in individuals suffering from bipolar disorder.
- Motivation enhancement – This is commonly expressed in the form of being more talkative, fidgety, or having increased interest in tasks. This effect is mild when compared to amphetamines or methylphenidates.
- Dream potentiation – Reports list that taking bupropion can lead to wild, vivid, and realistic dreams, usually feeling linear and very immersive, almost like a fun adventure. Time also seems to have passed much more than it actually has from sleep to wake. It is also easier to recall dreams. Consequently, bupropion can also inhibit sleep, but this can be countered with melatonin safely. This effect is likely exerted by its antagonistic action on nicotinic acetylcholine receptors.
- Time distortion – This is in the form of time expansion. A time period such as twenty minutes can feel as if it were up to eight hours. It happens at unreasonably high doses.
- Increased music appreciation
- Immersion enhancement
- Cognitive euphoria – The euphoria produced by bupropion is usually mild but in some people it has been reported to produce intense euphoria on par with that of amphetamine.
- Ego inflation
- Dysphoria – This effect is only present at high doses, usually due to its deliriant actions.
- Novelty enhancement
- Language suppression – This effect is only present at high doses, usually due to its deliriant actions.
- Increased sense of humor
- Increased libido – Bupropion is sometimes prescribed off-label for treatment of SSRI-induced sexual dysfunction.
- Craving suppression – Bupropion reduces the enjoyment and therefore the need for nicotine. Alone or with varenicline, bupropion SR and ER can be used for treatment of tobacco addiction and dependence.
Auditory effects:
- Auditory hallucinations – This effect is only present at high doses, usually due to its deliriant actions.
- Auditory enhancement – Sounds may be easier or more painful to hear. Usually, this isn’t part of delirium necessarily, but it can be.
Toxicity and harm potential [4, 6]
Using harm reduction practices when taking bupropion is highly advised as the drug can lead to seizures. It is not recommended to combine bupropion with other substances that lower the seizure threshold, such as tramadol, or take it during GABAergic withdrawal. Even though the LD50 of bupropion is relatively average for rats and mice, it can still be extremely dangerous in overdose due to the risk of monoamine flood, seizures, and heart attacks or strokes.
Street Names, Prices and Approximate Dosage [4]
Bupropion, also known as “poor man’s cocaine,” is a prescription medication marketed under the brand name Wellbutrin. When obtained illegally, it can be sold on the street for prices ranging from $2 to $90 per pill. The website StreetRX tracks average street prices for illicit prescription drugs and reports that in 2022, Wellbutrin was reported as costing up to $90 per 150 mg pill.
It is important to note that bupropion can cause seizures, especially at high doses, and should not be combined with other substances that lower the seizure threshold, such as tramadol, or used during GABAergic withdrawal. The recommended dosage for immediate-release bupropion is as follows: threshold – 75 mg; light – 75-125 mg; common – 125-225 mg; strong – 225-325 mg; and heavy – 325 mg or more. However, heavy usage carries a high risk of death due to seizures. The duration of bupropion’s effects varies, with the total duration lasting 8-12 hours, onset occurring in 40-60 minutes, peak effects at 90 minutes, offset taking 5-8 hours, and after-effects lasting 1-2 days.
Dangerous interactions [4, 8, 9]
- Stimulants (Amphetamine, lisdexamfetamine, methylphenidate, cocaine) – This combination can increase the chance of a heart attack, stroke, or adrenergic flood. These agents often individually lowers the seizure threshold and may have additive effects when combined with Bupropion.
- Tramadol, Tapentadol, or any other drug or substance that lowers the seizure threshold such as dextropropoxyphene or lithium. – This combination can increase the risk of seizures, death from seizures, or status epilepticus (seizure lasting longer than five minutes).
- Sedatives (Alprazolam, clonazolam, diazepam, opioids, phenobarbital, secobarbital, quetiapine) – Bupropion’s effects are masked by sedatives such as benzodiazepines, barbiturates, alcohol, and antipsychotics. If the effects of sedatives wear off before bupropion’s, bupropion’s effects may seem or become more pronounced.
- Alcohol – This combination increases the risk of atypical and unpleasant or dangerous side effects such as seizures, paranoia, or depression.
- DXM – Bupropion is a potent inhibitor of CYP2D6, the enzyme primarily responsible for breaking down DXM. This can lead to prolonged effects and excessive accumulation of DXM in the bloodstream and both substances raise heart rate, in extreme cases, panic attacks caused by these substances have led to more serious heart issues.
- Cannabis – Bupropion causes anxiety, thought loops and paranoia more often than other stimulants.
- Caffeine – This combination of stimulants is generally considered unnecessary and may increase strain on the heart, as well as potentially causing anxiety and physical discomfort.
- Ketamine – Combining amphetamine and ketamine may result in psychoses that resemble schizophrenia, but not worse than the psychoses produced by either substance alone, but this is debatable. This is due to amphetamines ability to attenuated the disruption of working memory caused by ketamine. Amphetamine alone may result in grandiosity, paranoia, or somatic delusions with little to no effect on negative symptoms. Ketamine, however, will result in thought disorders, disruption of executive functioning, and delusions due to a modification of conception. These mechanisms are due to an increase of dopaminergic activity in the mesolimbic pathway caused by amphetamine due to its pharmacology effecting dopamine, and due to a disruption of dopaminergic functioning in the mesocortical pathways via NMDA antagonism effects of ketamine. Combining the two, you may expect mainly thought disorder along with positive symptoms.
- PCP – Increases risk of tachycardia, hypertension, and manic states.
- Methoxetamine – Increases risk of tachycardia, hypertension, and manic states.
- Psychedelics (e.g. LSD, mescaline, psilocybin) – Bupropion significantly increases risk of anxiety, paranoia, and thought loops.
- 25x-NBOMe – Amphetamines and NBOMes both provide considerable stimulation that when combined they can result in tachycardia, hypertension, vasoconstriction and, in extreme cases, heart failure. The anxiogenic and focusing effects of stimulants are also not good in combination with psychedelics as they can lead to unpleasant thought loops. NBOMes are known to cause seizures and stimulants can increase this risk.
- 2C-T-x – Suspected of mild MAOI properties. May increase the risk of hypertensive crisis.
- 5-MeO-xxT – Suspected of mild MAOI properties. May increase the risk of hypertensive crisis.
- DOx
- aMT – aMT has MAOI properties which may interact unfavorably with amphetamines.
- MAOIs – MAO-B inhibitors can increase the potency and duration of phenethylamines unpredictably. MAO-A inhibitors with amphetamine can lead to hypertensive crises.
Legal Status [1]
Bupropion is typically available by prescription only and is not usually classified as a controlled substance internationally. However, in Russia, it is banned as a narcotic drug, not because it is considered one in itself, but because it is a derivative of methcathinone. In Australia, France, and the UK, the only approved use for bupropion is for smoking cessation, and there are no generic versions available.
Synthesis of 2-(tert-butylamino)-1-(3-chlorophenyl)propan-1-one [10, 11]
Bupropion belongs to the cathinone class of molecules and is characterized by a substituted chlorine atom at R3 of its phenyl ring and a tert-butylamine at the amino group. Cathinones are a type of amphetamines that share a common amphetamine structure, consisting of a phenyl ring bound to an amino group (NH2) via an ethyl chain and an additional methyl substitution at Rα. Bupropion and other cathinones are distinguished by their ketone substitution on the beta carbon of the amphetamine skeleton, making them β-keto-amphetamines.
Various methods for synthesizing bupropion can be found in the literature.
Synthesis I. m-Chlorobenzonitrile is reacted with ethyl Grignard reagent in ether to produce m-chlorobenzyl ethyl ketone, which is brominated in dichloromethane. The product is reacted with tertiary butyl amine in acetonitrile to yield bupropion base. Treatment of an ethereal solution of the base with dry HCl yields the salt. Scheme in Figure 5.
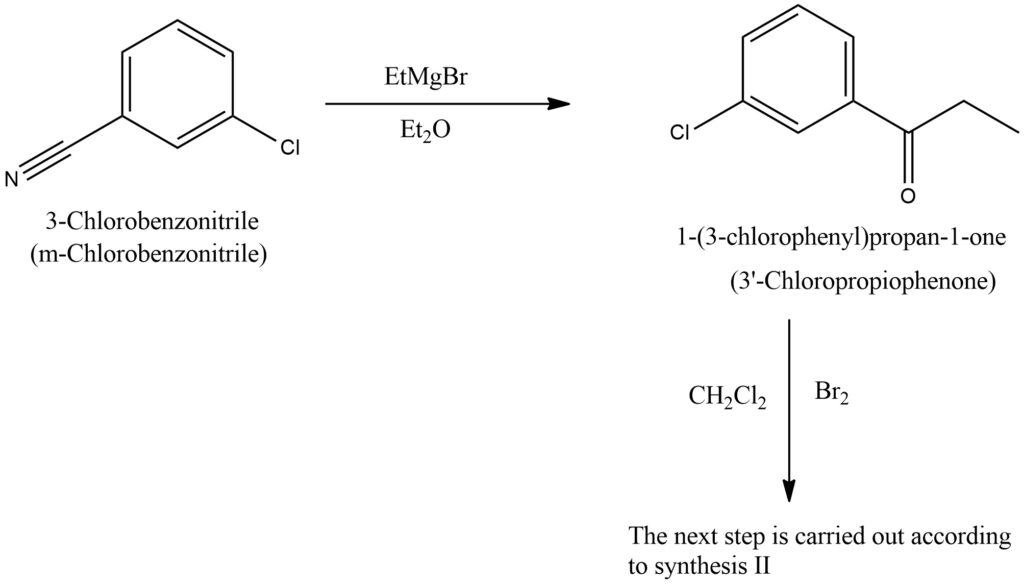
Figure 5. General scheme of Synthesis I 2-(tert-butylamino)-1-(3-chlorophenyl)propan-1-one synthesis.
The synthesis II of bupropion can be achieved through various methods, including the synthesis starting from m-chloropropiophenone as shown in Figure 6.
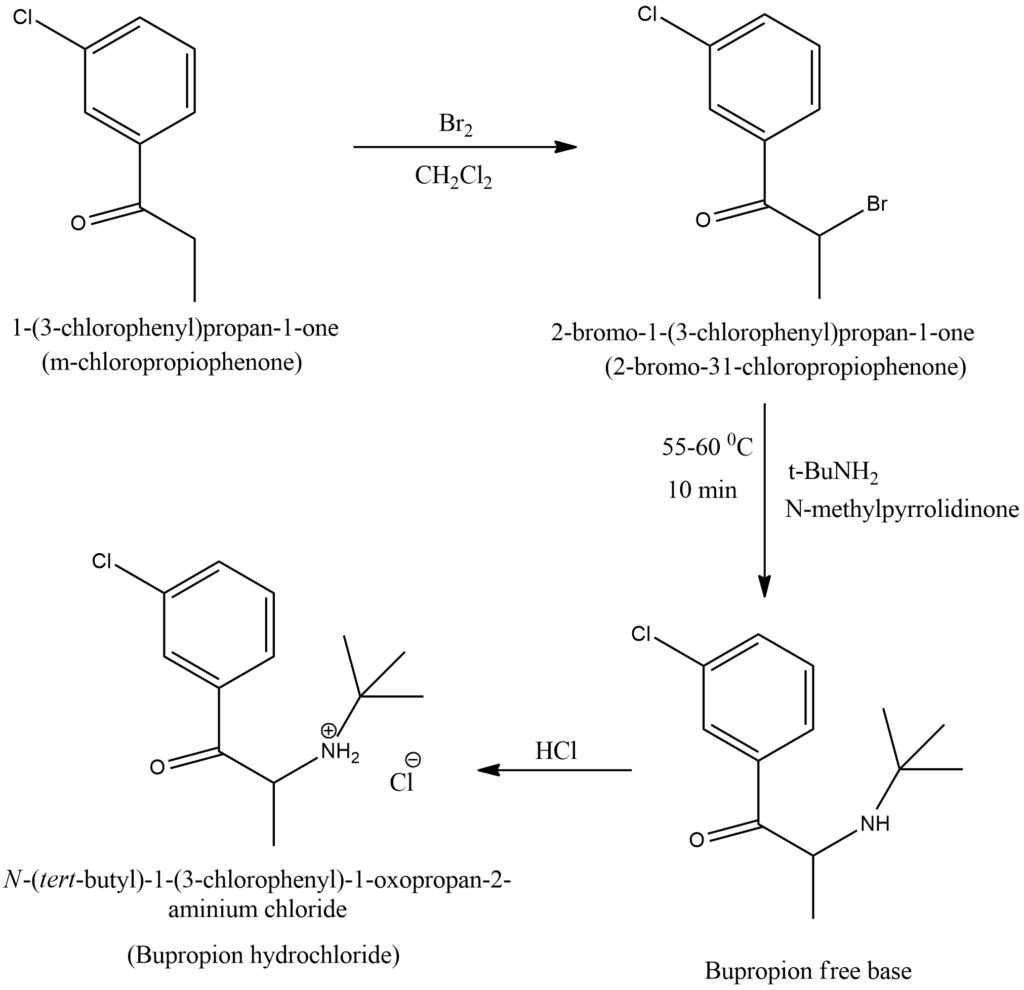
Figure 6. General scheme of Synthesis II 2-(tert-butylamino)-1-(3-chlorophenyl)propan-1-one synthesis
Conclusion
Bupropion is a member of the cathinone class and is primarily used as an atypical antidepressant for major depressive disorder and smoking cessation support. It stands out from other antidepressants due to its unique features. However, it is essential to be aware of potential side effects and drug interactions before using this medication. Various methods of synthesizing bupropion can be found in literature. The drug was first synthesized by Nariman Mehta of Burroughs Wellcome (now GlaxoSmithKline) in 1969, granted a US patent in 1974, and approved by the FDA as an antidepressant on December 30, 1985, marketed under the name Wellbutrin. It is highly recommended to use harm reduction practices while taking bupropion due to its potential to cause seizures. Combining bupropion with other substances that lower the seizure threshold, such as tramadol, or taking it during GABAergic withdrawal is not advised. Although the LD50 of bupropion is average for rats and mice, it can still be incredibly dangerous in overdose due to the risk of monoamine flood, seizures, and heart attacks or strokes.
Bibliography
- https://pubchem.ncbi.nlm.nih.gov/compound/444#section=Depositor-Supplied-Synonyms
- https://en.wikipedia.org/wiki/Bupropion
- https://www.chemspider.com/Chemical-Structure.431.html
- https://psychonautwiki.org/wiki/Bupropion
- Jon O. Ebbert, Dorothy K. Hatsukami etc. Combination Varenicline and Bupropion SR for Tobacco Dependence Treatment in Cigarette Smokers: A Randomized Trial. JAMA, 2014, 311, 2, pp. 155–163. doi: 10.1001/jama.2013.283185 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3959999/
- Cayman Chemicals. Safety Data Sheet of Bupropion. https://cdn.caymanchem.com/cdn/msds/10488m.pdf
- Susan J. Keam Dextromethorphan/Bupropion: First Approval. Keam, S.J. Dextromethorphan/Bupropion: First Approval. CNS Drugs, 2022, 36, pp. 1229–1238. https://doi.org/10.1007/s40263-022-00968-4 https://link.springer.com/article/10.1007/s40263-022-00968-4
- Michael Kotlyar, Lisa H Brauer etc. Inhibition of CYP2D6 activity by bupropion. J Clin Psychopharmacol, 2005, 25, 3, pp. 226-9. doi: 10.1097/01.jcp.0000162805.46453.e3 https://pubmed.ncbi.nlm.nih.gov/15876900/
- John H. Krystal, Edward B. Perry etc. Comparative and Interactive Human Psychopharmacologic Effects of Ketamine and Amphetamine. Implications for Glutamatergic and Dopaminergic Model Psychoses and Cognitive Function. Arch Gen Psychiatry, 2005, 62, 9, pp. 985-995. doi:10.1001/archpsyc.62.9.985 https://jamanetwork.com/journals/jamapsychiatry/fullarticle/1108408
- Troy, D.B. (Ed); Remmington The Science and Practice of Pharmacy. 21 st Edition. Lippincott Williams & Williams, Philadelphia, PA 2005, p. 1519. https://www.worldcat.org/title/remington-the-science-and-practice-of-pharmacy/oclc/224307481
- Perrine, D. M., Ross, J. T., Nervi, S. J., & Zimmerman, R. H. A Short, One-Pot Synthesis of Bupropion (Zyban, Wellbutrin). Journal of Chemical Education, 2000, 77, 11, p. 1479. doi:10.1021/ed077p1479 https://pubs.acs.org/doi/abs/10.1021/ed077p1479