
Abstract
Sildenafil, a phosphodiesterase 5 inhibitor, urological agent, and vasodilator agent, was originally synthesized by a team of pharmaceutical chemists at Pfizer’s research facility in Sandwich, Kent, England. Initially studied for its potential use in treating hypertension and angina pectoris, it was during Phase I clinical trials led by Ian Osterloh at Morriston Hospital in Swansea that the drug’s unexpected effect on inducing penile erections was discovered. Pfizer made the strategic decision to market sildenafil for erectile dysfunction, which later became a widely-cited example of drug repositioning. Sildenafil was patented in 1996 and approved by the FDA for treating erectile dysfunction on March 27, 1998, becoming the first oral treatment for this condition in the United States. It was subsequently launched for sale later that year, and its annual sales peaked at US$1.934 billion in 2008. Sold under the brand name Viagra, among others, sildenafil is also used to treat pulmonary arterial hypertension. Its efficacy in treating sexual dysfunction in women remains unclear. This article provides a comprehensive overview of sildenafil, including its general information, physico-chemical properties, pharmacology in recreational use, effects and symptoms, hepatotoxicity, other names (generics), prices and approximate dosage, dangerous interactions, legal status, synthesis of 5-[2-ethoxy-5-(4-methylpiperazin-1-yl)sulfonylphenyl]-1-methyl-3-propyl-6H-pyrazolo[4,3-d]pyrimidin-7-one, conclusion, and bibliography.

Sildenafil Citrate Tablet – Drug Information
General Information About Sildenafil [1-4]
Other synonyms names of Sildenafil are: 5-(2-Ethoxy-5-((4-methylpiperazin-1-yl)sulfonyl)phenyl)-1-methyl-3-propyl-1H-pyrazolo[4,3-d]pyrimidin-7(6H)-one; 5-{2-(ethyloxy)-5-[(4-methylpiperazin-1-yl)sulfonyl]phenyl}-1-methyl-3-propyl-1,6-dihydro-7H-pyrazolo[4,3-d]pyrimidin-7-one
IUPAC Name of Sildenafil: 5-[2-ethoxy-5-(4-methylpiperazin-1-yl)sulfonylphenyl]-1-methyl-3-propyl-6H-pyrazolo[4,3-d]pyrimidin-7-one
CAS numbers are 139755-83-2; 171599-83-0 (citrate)
Trade names are VIAGRA; Aphrodil; Vizarsin; Patrex; Sildenafil teva
Physico-Chemical Properties of Sildenafil [1-4]
- Molecular Formula C22H30N6O4S
- Molar Weight 474.6 g/mol
- Boiling point 672.4 °C
- Melting Point 187-190 °C
- Solubility: In water, 4.665 mg/L at 25 °C (est); 100 mM in DMSO; 100 mM in ethanol
- Form: Crystals
Structural formula present on Figure 1.
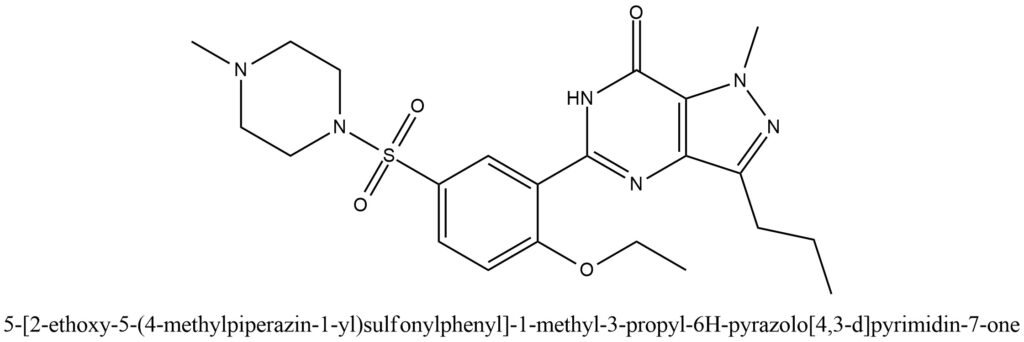
Figure 1. Structure of Sildenafil
Commercial possible of the Sildenafil can be seen in the pictures provided in Figure 2 and Figure 3.

Figure 2. Commercial Viagra
Figure 3. Commercial Sildenafil
General Information of Sildenafil in Pharmacology [5-10]
Figure 4. Sildenafil in Use
How Long Does Viagra Last?
In vitro studies have demonstrated that sildenafil exhibits selectivity towards phosphodiesterase-5 (PDE5) over other phosphodiesterases. Notably, it is 10 times more potent in inhibiting PDE5 than PDE6, which plays a role in retinal phototransduction. Sildenafil also exhibits selectivity over PDE1 (80 times), PDE2, PDE3, PDE4, PDE7, PDE8, PDE9, PDE10, and PDE11 (over 700 times). Additionally, sildenafil has more than 4,000 times selectivity for PDE5 over PDE3, which is involved in the regulation of cardiac contractility.
Several double-blind, placebo-controlled crossover studies have evaluated the efficacy of sildenafil in patients with organic or psychogenic erectile dysfunction. Objective measurements of hardness and duration of erections using RigiScan® showed improved erectile response after sildenafil administration compared to placebo, with most studies assessing efficacy approximately 60 minutes after dosing. The erectile response generally increased with higher sildenafil doses and plasma concentrations. In one study, the effect was observed for up to 4 hours, but with diminished response compared to 2 hours.
Sildenafil has mild and transient effects on systemic blood pressure, usually not resulting in clinical effects. Chronic dosing of 80 mg, three times a day in patients with systemic hypertension resulted in a mean decrease of 9.4 mmHg in systolic blood pressure and 9.1 mmHg in diastolic blood pressure from baseline. In patients with pulmonary arterial hypertension, lesser effects on blood pressure reduction (2 mmHg in both systolic and diastolic pressure) were observed with chronic dosing of 80 mg, three times a day, while no reductions were seen at the recommended dose of 20 mg, three times a day.
Single oral doses of sildenafil up to 100 mg in healthy volunteers did not produce clinically relevant effects on ECG. Chronic dosing of 80 mg, three times a day in patients with pulmonary arterial hypertension also showed no clinically relevant effects on ECG. In patients with severe coronary artery disease, a single oral dose of 100 mg sildenafil resulted in a decrease of 7% in mean resting systolic blood pressure and 6% in diastolic blood pressure compared to baseline, with a 9% decrease in mean pulmonary systolic blood pressure. However, sildenafil did not affect cardiac output or blood flow through stenosed coronary arteries.
Some subjects experienced mild and transient differences in color discrimination (blue/green) using the Farnsworth-Munsell 100 hue test at 1 hour after a 100 mg dose of sildenafil, with no effects observed after 2 hours post-dose. This change in color discrimination is postulated to be related to the inhibition of PDE6, which is involved in retinal phototransduction. Sildenafil did not affect visual acuity or contrast sensitivity in a small placebo-controlled study of patients with early age-related macular degeneration (n = 9), as assessed by various visual tests including visual acuity, Amsler grid, color discrimination simulated traffic light, and the Humphrey perimeter and photostress test.
Crystal structure of human PDE5 with bound sildenafil (Figure 5).
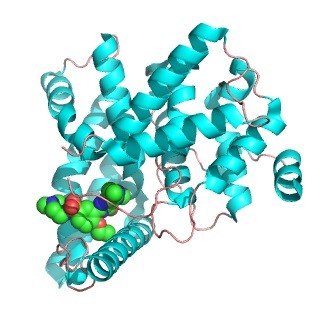
Figure 5. Crystal structure of human PDE5 with bound sildenafil [5]
Recreational Use
The popularity of sildenafil, known by its trade name Viagra, among young adults has grown over time. While the drug is primarily used for treating erectile dysfunction, it has also gained recreational use. Some individuals believe that sildenafil can increase libido, improve sexual performance, or even permanently enhance penis size, leading to its recreational use. However, limited studies suggest that sildenafil may have little effect on those without erectile dysfunction. In one study, a 25 mg dose did not significantly change erectile quality, but did reduce the postejaculatory refractory time. It is important to note that a significant placebo effect was observed in the control group. Furthermore, sildenafil and other PDE5 inhibitors are often used recreationally without prescription, particularly among users of illegal drugs, in an attempt to counteract the effects of other substances.
Toxicity
Adverse reactions in single-dose volunteer studies of sildenafil at doses up to 800 mg were similar to those seen at lower doses, but with increased incidence rates and severities. Doses of 200 mg did not result in increased efficacy, but did show increased incidence of adverse reactions such as headache, flushing, dizziness, dyspepsia, nasal congestion, and altered vision. Sildenafil is not recommended for women of childbearing potential unless also using appropriate contraceptive measures, due to lack of data on its effects in pregnant women being treated for pulmonary arterial hypertension (PAH). Safety and efficacy of sildenafil during labor and delivery in treating PAH have not been studied. Caution should be exercised when administering sildenafil to nursing women as it is unknown if sildenafil or its metabolites are excreted in human breast milk. Safety and efficacy of sildenafil for treating PAH in children below 1 year of age has not been established due to lack of available data. Clinical experience with elderly patients using sildenafil for PAH has varied, with some reports suggesting no identified differences in responses between elderly and younger patients, while others have documented potential decreased clinical efficacy in elderly patients as measured by 6-minute walk distance. Dose selection for elderly patients should be cautious, taking into consideration decreased hepatic, renal, or cardiac function, and concomitant disease or drug therapy. However, when sildenafil was used to treat erectile dysfunction in healthy elderly volunteers (65 years or over), reduced clearance of sildenafil was observed, resulting in about 90% higher plasma concentrations of sildenafil and its active N-desmethyl metabolite compared to younger volunteers (18-45 years). This increase in free sildenafil plasma concentration was approximately 40% due to age-differences in plasma protein binding. Sildenafil was not found to be carcinogenic in rats or mice in various in vivo and in vitro assays to detect mutagenicity or clastogenicity. Fertility was not impaired in rats given sildenafil up to 60 mg/kg/day for 36 days in females and 102 days in males, a dose producing an AUC value of more than 25 times the human male AUC. There have been rare reports of acute liver injury attributed to sildenafil use, with unclear latency periods due to intermittent and sometimes unacknowledged use of the drug. The pattern of serum enzyme elevations in reported cases has ranged from hepatocellular to cholestatic, with some cases evolving from one to the other. The most convincing cases have shown mild cholestatic or “mixed” hepatitis occurring within 1 to 3 months of starting sildenafil, without immunoallergic features or autoantibodies observed. There have also been instances of acute onset with high serum aminotransferase levels that have characteristics of ischemic injury or anabolic steroid use. In two cases, re-exposure to sildenafil did not result in recurrence. Overall, the hepatotoxicity of sildenafil is not well established and appears to be rare, if it occurs at all.
Effects and symptoms of Sildenafil Use
During clinical trials, sildenafil use was associated with various adverse effects, such as headache, flushing, indigestion, nasal congestion, and impaired vision, including photophobia and blurred vision. Some users even reported seeing a blue tint (cyanopsia) in everything, which can be explained by sildenafil’s minor selectivity for PDE6, the phosphodiesterase found in the retina. This can result in color vision abnormalities, blurriness, and loss of peripheral vision. In July 2005, the U.S. Food and Drug Administration (FDA) updated the labeling for Cialis, Levitra, and Viagra to reflect rare post-marketing reports of sudden vision loss. However, the FDA acknowledged that it is difficult to determine whether these erectile dysfunction medications were the cause of the vision loss or if other factors such as high blood pressure or diabetes, or a combination of these issues, were involved. A thorough review of pooled data from clinical trials, which included well-documented information about the dose and duration of drug exposure for a large number of patients, found no evidence of increased risk of non-arteritic anterior ischemic optic neuropathy or other adverse ocular events associated with the use of PDE-5 inhibitors. Rare but serious adverse effects, identified through post-marketing surveillance, include prolonged erections, severe low blood pressure, myocardial infarction (heart attack), ventricular arrhythmias, stroke, increased intraocular pressure, and sudden hearing loss. In October 2007, the FDA announced that the labeling for all PDE5 inhibitors, including sildenafil, must include a more prominent warning about the potential risk of sudden hearing loss.

Erections Gone Wrong: What Viagra Does to the Penis
Other Names (Generics), Prices and Approximate Dosage
Other brand names for sildenafil include Aronix, Liberize, Nipatra, Revatio, and Grandipam. VIAGRA, which is one of the most counterfeited drugs worldwide, is often sold as cheap knockoffs that are illegal and potentially harmful. It’s difficult to determine their origin or contents. The cost of sildenafil oral tablets at a dosage of 100 mg is approximately $19 for a supply of 10 tablets.
Sildenafil is known to be rapidly absorbed, with maximum plasma concentrations typically reached within 30-120 minutes (median of 60 minutes) after oral administration in a fasting patient. The mean absolute bioavailability of sildenafil is about 41% (range of 25-63%). After oral dosing three times a day, the area under the concentration-time curve (AUC) and maximum plasma concentration (Cmax) increase proportionally with the dose within the recommended range of 25-100 mg. However, in patients with pulmonary arterial hypertension, the oral bioavailability of sildenafil was approximately 43% higher on average with a dosing regimen of 80 mg three times a day compared to lower doses. Administration of sildenafil with food can decrease the rate of absorption, with a mean delay in time to maximum concentration (Tmax) of about 60 minutes and a mean decrease in Cmax of approximately 29%. However, the extent of absorption is not significantly affected, with only a decrease of about 11% observed in the AUC. The terminal half-life of sildenafil is approximately 3 to 5 hours. For adults up to 65 years of age, the recommended oral dosage of sildenafil is 50 mg as a single dose, no more than once a day, taken 1 hour before sexual intercourse. Alternatively, the medicine may be taken 30 minutes to 4 hours before sexual intercourse. For adults 65 years of age and older, the recommended dosage is 25 mg as a single dose, no more than once a day, taken 1 hour before sexual intercourse. Alternatively, the medicine may be taken 30 minutes to 4 hours before sexual intercourse.
Dangerous interactions
Sildenafil, along with other phosphodiesterase (PDE) type 5 inhibitors like tadalafil and vardenafil, significantly enhances the vasodilatory effects of organic nitrates and nitrites, such as nitroglycerin and isosorbide dinitrate, leading to a reduction in systolic blood pressure by more than 25 mm Hg in the case of sildenafil. This can result in life-threatening hypotension and hemodynamic compromise. Nitrates and nitrites stimulate guanylate cyclase, promoting the formation of cyclic guanosine monophosphate (cGMP), while PDE type 5 inhibitors inhibit the degradation of cGMP by phosphodiesterase (PDE) type 5, leading to increased accumulation of cGMP and more pronounced smooth muscle relaxation and vasodilation compared to using either PDE type 5 inhibitors or nitrates/nitrites alone. This interaction is likely to occur with any organic nitrate, nitrite, or nitric oxide donor, regardless of their predominant hemodynamic site of action. Combining sildenafil with Grapefruit Juice and Pomelo Juice may also increase the risk of certain side effects. Some users may mix sildenafil with methylenedioxymethamphetamine (MDMA, ecstasy), other stimulants, or opiates to counteract the common side effect of erectile dysfunction, a combination known as “sextasy”, “rockin’ and rollin'” or “trail mix”. However, mixing sildenafil with amyl nitrite, another vasodilator, is particularly dangerous and potentially fatal.
Legal Status
- Australia: Schedule 4 (Prescription only)
- Canada: Prescription only
- United Kingdom: P (Pharmacy medicines) / POM
- United States: Prescription only
- European Union: Prescription only
- In general: Prescription only
Synthesis of 5-[2-ethoxy-5-(4-methylpiperazin-1-yl)sulfonylphenyl]-1-methyl-3-propyl-6H-pyrazolo[4,3-d]pyrimidin-7-one [11]
The commercial synthesis of sildenafil citrate is outlined in scheme on Figure 6.
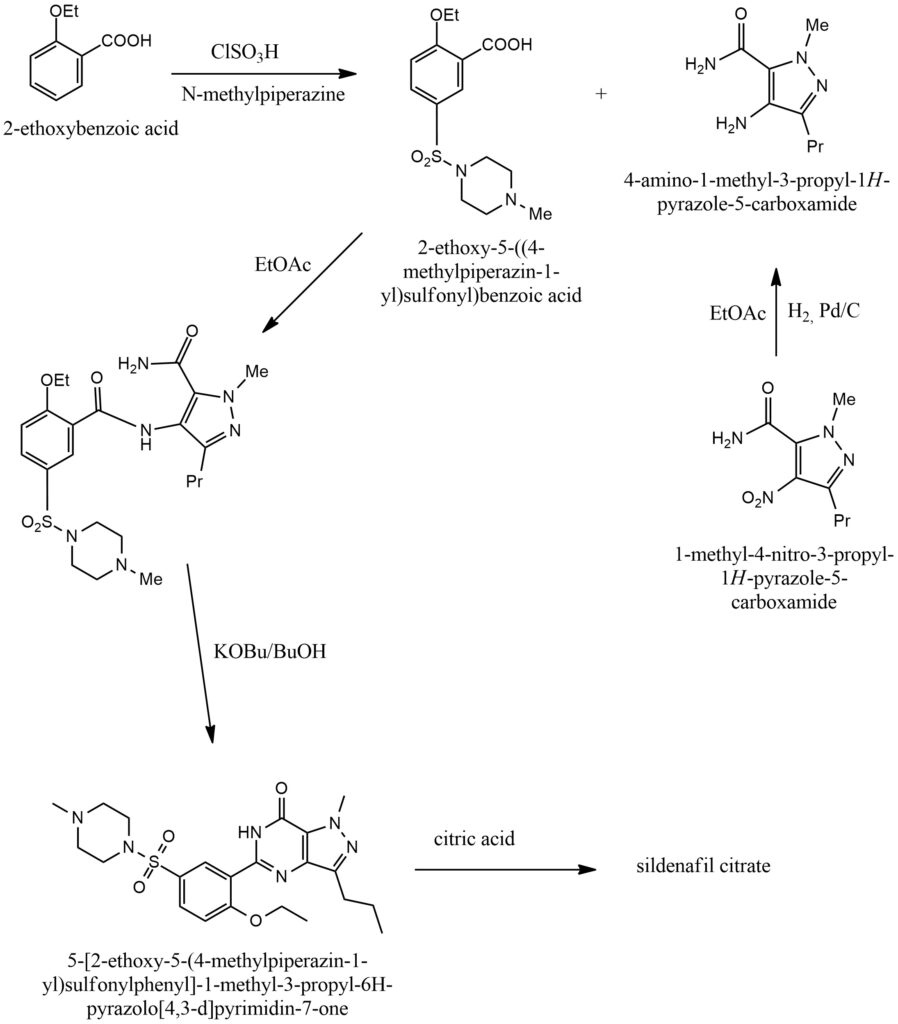
Figure 6. Commercial synthesis of sildenafil citrate
Conclusion
Sildenafil, a medication categorized as a Phosphodiesterase Inhibitor, Urological Agent, and Vasodilator Agent, is commonly known by its brand name Viagra. It is primarily used for the treatment of erectile dysfunction and pulmonary arterial hypertension. Over the years, sildenafil has gained popularity among young adults. Its trade name, Viagra, is widely recognized in popular culture, and the drug has been associated with recreational use due to its reputation in treating erectile dysfunction. Some individuals believe that sildenafil can increase libido, improve sexual performance, or permanently enhance penis size. Limited studies on the recreational use of sildenafil suggest that it may have little effect in individuals without erectile dysfunction. However, some users may mix sildenafil with other substances such as methylenedioxymethamphetamine (MDMA, ecstasy), other stimulants, or opiates in an attempt to counteract the common side effect of erectile dysfunction, a combination known as “sextasy”, “rockin’ and rollin'”, or “trail mix”. It is important to note that mixing sildenafil with amyl nitrite, another vasodilator, can be extremely dangerous and potentially fatal. It is also worth mentioning that Viagra is one of the most counterfeited drugs worldwide.
Bibliography
- https://en.wikipedia.org/wiki/Sildenafil
- https://pubchem.ncbi.nlm.nih.gov/compound/135398744
- https://www.chemspider.com/Chemical-Structure.5023.html
- https://go.drugbank.com/drugs/DB00203
- Sung, BJ., Yeon Hwang, K., Ho Jeon, Y. et al. Structure of the catalytic domain of human phosphodiesterase 5 with bound drug molecules. Nature 425, 98–102 (2003). https://doi.org/10.1038/nature01914 https://www.nature.com/articles/nature01914
- https://www.drugs.com/cons/sildenafil.html
- Eva Ausó, Violeta Gómez-Vicente Visual Side Effects Linked to Sildenafil Consumption: An Update. Biomedicines, 2021, 9, 3, p. 291. https://doi.org/10.3390/biomedicines9030291 https://www.mdpi.com/2227-9059/9/3/291
- Trond J. Cooper, John G.F. Cleland Effects of sildenafil on symptoms and exercise capacity for heart failure with reduced ejection fraction and pulmonary hypertension (the SilHF study): a randomized placebo-controlled multicentre trial. European Journal of Heart Failure, 2022, Volume24, Issue7, pp. 1239-1248. https://doi.org/10.1002/ejhf.2527 https://onlinelibrary.wiley.com/doi/full/10.1002/ejhf.2527
- Nazir Muhammad Hashir; Ahmad Muhammad1; Azeem Saleha Is recreational use of sildenafil a new trend? Annals of Medicine & Surgery, 2022, 82. DOI: 10.1016/j.amsu.2022.104659 https://journals.lww.com/annals-of-medicine-and-surgery/Fulltext/2022/10000/Is_recreational_use_of_sildenafil_a_new_trend_.125.aspx
- Jay Narayan Pandit, Ruchi Kumari Rare fatal effect of combined use of sildenafil and alcohol leading to Cerebrovascular Accident. Journal of Forensic and Legal Medicine, 2023, Volume 95, p. 102504. https://doi.org/10.1016/j.jflm.2023.102504 https://www.sciencedirect.com/science/article/abs/pii/S1752928X23000227
- Peter J. Dunn Synthesis of Commercial Phosphodiesterase(V) Inhibitors. Org. Process Res. Dev., 2005, 9, 1, pp. 88–97. https://doi.org/10.1021/op040019c https://pubs.acs.org/doi/10.1021/op040019c